Blank 3 1 Health Care Directive PDF Template
Navigating through the intricacies of planning for future healthcare decisions can seem daunting, yet it's an essential step in ensuring one's wishes are respected and executed. Among the tools at our disposal for such planning, the Form 3-1 Advance Health Care Directive holds significant importance. This document empowers individuals to designate a trusted person, or agent, to make healthcare decisions on their behalf should they become unable to do so, covering a broad array of decisions from the consent or refusal of medical treatment to the management of diet and hydration. Additionally, it offers the option to outline specific healthcare wishes directly, without appointing an agent, giving one the space to express their preferences regarding life-prolonging treatments, pain management, and even the donation of organs posthumously. It emphasizes open communication with chosen agents to ensure they understand and are willing to uphold the individual’s healthcare desires. The directive serves as a robust foundation to safeguard one's healthcare preferences, illustrating the importance of thoughtful preparation in healthcare decision-making. Its dual functionality, covering both the delegation of decision-making power and the expression of individual healthcare directives, underlines the document’s flexibility and adaptability to a range of personal healthcare planning philosophies and requirements.
Preview - 3 1 Health Care Directive Form
FORM 3 - 1
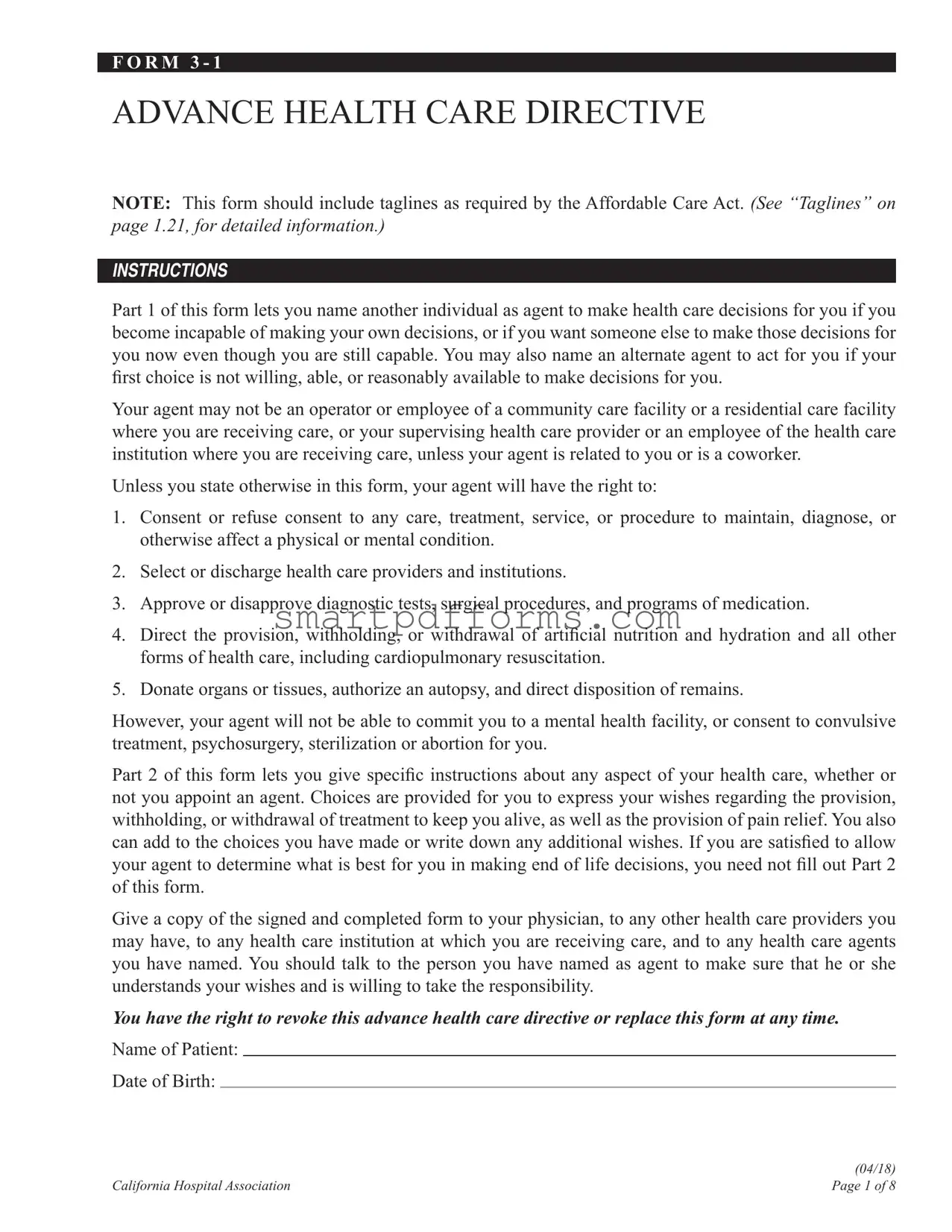
ADVANCE HEALTH CARE DIRECTIVE
NOTE: This form should include taglines as required by the Affordable Care Act. (See “Taglines” on page 1.21, for detailed information.)
INSTRUCTIONS
Part 1 of this form lets you name another individual as agent to make health care decisions for you if you become incapable of making your own decisions, or if you want someone else to make those decisions for
you now even though you are still capable. You may also name an alternate agent to act for you if your irst choice is not willing, able, or reasonably available to make decisions for you.
Your agent may not be an operator or employee of a community care facility or a residential care facility where you are receiving care, or your supervising health care provider or an employee of the health care institution where you are receiving care, unless your agent is related to you or is a coworker.
Unless you state otherwise in this form, your agent will have the right to:
1.Consent or refuse consent to any care, treatment, service, or procedure to maintain, diagnose, or otherwise affect a physical or mental condition.
2.Select or discharge health care providers and institutions.
3.Approve or disapprove diagnostic tests, surgical procedures, and programs of medication.
4.Direct the provision, withholding, or withdrawal of artiicial nutrition and hydration and all other forms of health care, including cardiopulmonary resuscitation.
5.Donate organs or tissues, authorize an autopsy, and direct disposition of remains.
However, your agent will not be able to commit you to a mental health facility, or consent to convulsive treatment, psychosurgery, sterilization or abortion for you.
Part 2 of this form lets you give speciic instructions about any aspect of your health care, whether or
not you appoint an agent. Choices are provided for you to express your wishes regarding the provision,
withholding, or withdrawal of treatment to keep you alive, as well as the provision of pain relief. You also can add to the choices you have made or write down any additional wishes. If you are satisied to allow your agent to determine what is best for you in making end of life decisions, you need not ill out Part 2
of this form.
Give a copy of the signed and completed form to your physician, to any other health care providers you may have, to any health care institution at which you are receiving care, and to any health care agents you have named. You should talk to the person you have named as agent to make sure that he or she understands your wishes and is willing to take the responsibility.
You have the right to revoke this advance health care directive or replace this form at any time.
Name of Patient:
Date of Birth:
(04/18)
California Hospital Association |
Page 1 of 8 |
Form
PART 1 – POWER OF ATTORNEY FOR HEALTH CARE
DESIGNATION OF AGENT:
I designate the following individual as my agent to make health care decisions for me: Name of individual you choose as agent:
Address:
Telephone:
(home phone) |
(work phone) |
(cell/pager) |
OPTIONAL: If I revoke my agent’s authority or if my agent is not willing, able, or reasonably available to make a health care decision for me, I designate as my irst alternate agent:
Name of individual you choose as irst alternate agent:
Address:
Telephone:
(home phone) |
(work phone) |
(cell/pager) |
OPTIONAL: If I revoke the authority of my agent and irst alternate agent or if neither is willing, able,
or reasonably available to make a health care decision for me, I designate as my second alternate agent: Name of individual you choose as second alternate agent:
Address:
Telephone:
(home phone) |
(work phone) |
(cell/pager) |
AGENT’S AUTHORITY:
My agent is authorized to make all health care decisions for me, including decisions to provide, withhold, or withdraw artiicial nutrition and hydration and all other forms of health care to keep me alive, except
as I state here:
(Add additional sheets if needed.)
(04/18)
Page 2 of 8 |
California Hospital Association |
Form
WHEN AGENT’S AUTHORITY BECOMES EFFECTIVE:
My agent’s authority becomes effective when my primary physician determines that I am unable to make my own health care decisions.
(Initial here)
OR
My agent’s authority to make health care decisions for me takes effect immediately.
(Initial here)
AGENT’S OBLIGATION:
My agent shall make health care decisions for me in accordance with this power of attorney for health care, any instructions I give in Part 2 of this form, and my other wishes to the extent known to my agent. To the extent my wishes are unknown, my agent shall make health care decisions for me in accordance with what my agent determines to be in my best interest. In determining my best interest, my agent shall consider my personal values to the extent known to my agent.
AGENT’S POSTDEATH AUTHORITY:
My agent is authorized to make anatomical gifts, authorize an autopsy and direct disposition of my remains, except as I state here or in Part 3 of this form:
(Add additional sheets if needed.)
NOMINATION OF CONSERVATOR:
If a conservator of my person needs to be appointed for me by a court, I nominate the agent designated in this form. If that agent is not willing, able or reasonably available to act as conservator, I nominate the alternate agents whom I have named, in the order designated.
(04/18)
California Hospital Association |
Page 3 of 8 |
Form
PART 2 – INSTRUCTIONS FOR HEALTH CARE
If you ill out this part of the form, you may strike any wording you do not want.
END OF LIFE DECISIONS:
I direct that my health care providers and others involved in my care provide, withhold, or withdraw treatment in accordance with the choice I have marked below:
Choice Not To Prolong Life:
(Initial here)
I do not want my life to be prolonged if (1) I have an incurable and irreversible condition that will result in my death within a relatively short time, (2) I become unconscious and, to a
reasonable degree of medical certainty, I will not regain consciousness, or (3) the likely risks and burdens of treatment would outweigh the expected beneits,
OR
Choice To Prolong Life:
(Initial here)
I want my life to be prolonged as long as possible within the limits of generally accepted health care standards.
RELIEF FROM PAIN:
Except as I state in the following space, I direct that treatment for alleviation of pain or discomfort be provided at all times, even if it hastens my death:
(Add additional sheets if needed.)
OTHER WISHES:
(If you do not agree with any of the optional choices above and wish to write your own, or if you wish to add to the instructions you have given above, you may do so here.) I direct that:
(Add additional sheets if needed.)
(04/18)
Page 4 of 8 |
California Hospital Association |
Form
PART 3 – DONATION OF ORGANS AT DEATH (OPTIONAL)
I. Upon my death:
I give any needed organs, tissues, or parts.
(Initial here)
OR
I do not authorize the donation of any organs, tissues or parts.
(Initial here)
OR
I give the following organs, tissues, or parts only:
(Initial here)
II.If you wish to donate organs, tissues, or parts, you must complete II. and III. My gift is for the following purposes:
Transplant |
|
|
Research |
|
|
|
|
|
(Initial here) |
|
(Initial here) |
||
Therapy |
|
|
Education |
|
||
|
(Initial here) |
|
(Initial here) |
|||
III.I understand that tissue banks work with both nonproit and
It is possible that donated skin may be used for cosmetic or reconstructive surgery purposes. It is possible that donated tissue may be used for transplants outside of the United States.
1. My donated skin may be used for cosmetic surgery purposes.
Yes |
|
No |
|
|
(Initial here) |
(Initial here) |
|
2. My donated tissue may be used for applications outside of the United States.
Yes |
|
No |
|
|
(Initial here) |
(Initial here) |
|
3.My donated tissue may be used by
Yes |
|
No |
|
|
(Initial here) |
(Initial here) |
|
(Health and Safety Code Section 7158.3)
(04/18)
California Hospital Association |
Page 5 of 8 |
Form
PART 4 – PRIMARY PHYSICIAN (OPTIONAL)
I designate the following physician as my primary physician:
Name of Physician:
Telephone:
Address:
OPTIONAL: If the physician I have designated above is not willing, able, or reasonably available to act as my primary physician, I designate the following physician as my primary physician:
Name of Physician:
Telephone:
Address:
PART 5 – SIGNATURE
The form must be signed by you and by two qualiied witnesses, or acknowledged before a notary public.
SIGNATURE:
Sign and date the form here:
Date: |
|
|
Time: |
|
AM / PM |
Signature: |
|
|
|
|
|
(patient)
Print name:
(patient)
Address:
STATEMENT OF WITNESSES:
I declare under penalty of perjury under the laws of California (1) that the individual who signed or acknowledged this advance health care directive is personally known to me, or that the individual’s identity was proven to me by convincing evidence, (2) that the individual signed or acknowledged this
advance directive in my presence, (3) that the individual appears to be of sound mind and under no duress, fraud, or undue inluence, (4) that I am not a person appointed as agent by this advance directive, and (5)
that I am not the individual’s health care provider, an employee of the individual’s health care provider, the operator of a community care facility, an employee of an operator of a community care facility, the operator of a residential care facility for the elderly, nor an employee of an operator of a residential care facility for the elderly.
(04/18)
Page 6 of 8 |
California Hospital Association |

|
|
|
|
|
|
|
|
|
|
Form |
|
FIRST WITNESS |
|
|
|
|
|
||||||
Name: |
|
|
|
|
|
|
|
Telephone: |
|
|
|
Address: |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
||
Date: |
|
|
|
Time: |
|
|
|
AM / PM |
|||
Signature: |
|
|
|
|
|
|
|
||||
|
|
|
|
|
(witness) |
|
|
|
|
|
|
Print name: |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
(witness) |
|
|
|
|
|
SECOND WITNESS |
|
|
|
|
|
||||||
Name: |
|
|
|
Telephone: |
|
||||||
Address: |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
||||||
Date: |
|
Time: |
|
|
|
AM / PM |
|||||
Signature: |
|
|
|
|
|
|
|||||
|
|
|
|
|
(witness) |
|
|
|
|
|
|
Print name: |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
(witness) |
|
|
|
|
|
ADDITIONAL STATEMENT OF WITNESSES:
At least one of the above witnesses must also sign the following declaration:
I further declare under penalty of perjury under the laws of California that I am not related to the individual executing this advance health care directive by blood, marriage, or adoption, and to the best of my knowledge, I am not entitled to any part of the individual’s estate upon his or her death under a will now existing or by operation of law.
Date: |
|
Time: |
|
AM / PM |
Signature:
(witness)
Print name:
(witness)
(04/18)
California Hospital Association |
Page 7 of 8 |
Form
A notary public or other oficer completing this certiicate veriies only the identity of the individual who signed the document to which this certiicate is attached, and not the truthfulness, accuracy,
or validity of the document.
YOU MAY USE THIS CERTIFICATE OF ACKNOWLEDGMENT BEFORE A NOTARY PUBLIC INSTEAD OF THE STATEMENT OF WITNESSES.
State of California |
) |
|
|
|
||||
County of |
|
|
|
) |
|
|
|
|
|
|
|
|
) |
|
|
|
|
On (date) |
|
|
before me, (name and title of the oficer) |
|
||||
|
|
|
|
|
|
personally appeared |
||
(name(s) of signer(s)) |
|
|
|
|
, who proved to |
|||
me on the basis of satisfactory evidence to be the person(s) whose name(s) is/are subscribed to the within instrument and acknowledged to me that he/she/they executed the same in his/her/their authorized capacity(ies), and that by his/her/their signature(s) on the instrument the person(s), or the entity upon behalf of which the person(s) acted, executed the instrument.
I certify under PENALTY OF PERJURY under the laws of the State of California that the foregoing paragraph is true and correct.
WITNESS my hand and oficial seal.
Signature:[Seal]
(notary)
PART
If you are a patient in a skilled nursing facility, the patient advocate or ombudsman must sign the following statement:
STATEMENT OF PATIENT ADVOCATE OR OMBUDSMAN
I declare under penalty of perjury under the laws of California that I am a patient advocate or ombudsman as designated by the State Department of Aging and that I am serving as a witness as required by Section 4675 of the Probate Code.
Date: |
|
Time: |
|
AM / PM |
Signature:
(patient advocate or ombudsman)
Print name:
(patient advocate or ombudsman)
Address:
(04/18)
Page 8 of 8 |
California Hospital Association |
Form Data
| Fact Number | Fact Detail |
|---|---|
| 1 | The Form 3-1 Advance Health Care Directive allows individuals to appoint an agent to make health care decisions on their behalf. |
| 2 | An alternate agent can be appointed if the primary agent is unable, unwilling, or not reasonably available to make decisions. |
| 3 | The designated agent has the authority to make a wide range of health care decisions unless specifically limited in the document. |
| 4 | This directive includes instructions for end-of-life care, including the decision between prolonging life or not, under certain medical conditions. |
| 5 | Individuals can specify their wishes regarding organ donation upon death in the directive. |
| 6 | The agent's authority becomes effective upon the principal's primary physician determining they are no longer able to make their own health care decisions or immediately if specified. |
| 7 | It gives options for the purpose of organ donation, such as transplant, research, therapy, or education. |
| 8 | The form explicitly states the agent cannot consent to mental health facility commitment, convulsive treatment, psychosurgery, sterilization, or abortion for the principal. |
| 9 | Part 2 of the form allows for detailed instructions about any aspect of one's health care, beyond appointing an agent. |
| 10 | Governed by the California Health and Safety Code Section 7158.3, the document includes guidelines regarding organ donation. |
Instructions on Utilizing 3 1 Health Care Directive
Filling out the 3-1 Health Care Directive form is a crucial step in ensuring your health care preferences are known and can be acted upon in the event you are unable to communicate them yourself. This document enables you to appoint an agent to make health care decisions on your behalf, specify your health care wishes, including end-of-life care, and make decisions about the donation of your organs after death. To complete this form accurately, follow the step-by-step instructions provided below.
- Designation of Agent:
- Enter your name and date of birth at the top of the form.
- Fill out the "Name of individual you choose as agent" section with your agent’s full name, address, and phone numbers (home, work, cell/pager).
- If applicable, fill out the information for your first and second alternate agents in the spaces provided.
- Agent’s Authority:
- Specify any limitations to your agent's authority in making health care decisions for you if you wish to impose any. If you need more space, add additional sheets as indicated.
- When Agent’s Authority Becomes Effective:
- Initial the appropriate box to indicate when your agent's authority becomes effective - either upon determination by your primary physician that you are unable to make your own health care decisions, or immediately.
- Agent’s Obligation:
- No action required here; this section outlines the responsibilities of your agent.
- Agent’s Postdeath Authority:
- Write any restrictions regarding post-death decisions such as organ donation, autopsy, or disposition of remains. Add additional sheets if needed.
- Nomination of Conservator:
- Review the nomination of your agent or alternate agents as conservator, if a conservatorship becomes necessary.
- Instructions for Health Care (Part 2):
- Specify your end-of-life treatment preferences by initialing either “Choice Not To Prolong Life” or “Choice To Prolong Life.”
- Provide directions about pain relief and any other health care wishes or add additional sheets if needed.
- Donation of Organs at Death (Part 3 - Optional):
- Indicate your organ donation preferences, the purposes for which your organs may be used, and your understanding regarding the use of donated tissues.
- Signature:
- Sign and date the form in the presence of the required witnesses or a notary, according to your state's laws.
After completing the form, ensure to give a copy to your physician, health care providers, the health care institution where you receive care, and the health care agents you have named. It's important to discuss your wishes with these individuals so they are prepared to honor your health care directives.
Obtain Answers on 3 1 Health Care Directive
What is a Form 3-1 Advance Health Care Directive and why is it important?
The Form 3-1 Advance Health Care Directive is a legal document that allows you to appoint someone else, known as an agent, to make health care decisions on your behalf if you become unable to make them yourself. This form is critical because it ensures that your health care preferences are known and respected, even if you lose the ability to communicate or make decisions. It encompasses decisions regarding medical treatments, surgical procedures, life support, and even organ donation after death. By filling out this form, you can have peace of mind knowing that your health care wishes will be honored.
Who can be designated as an agent in the Advance Health Care Directive?
You can designate almost any adult as your agent, including a family member, friend, or someone else you trust to make health care decisions on your behalf. However, there are specific restrictions to prevent conflicts of interest. For example, the operator or employee of a community care or residential care facility where you are receiving care cannot be your agent unless they are related to you or are a coworker. The importance of choosing someone who understands your values and wishes cannot be overstated, as this person may one day make critical health care decisions for you.
When does the agent's authority to make health care decisions for me become effective?
The agent's authority to make health care decisions on your behalf can become effective under two primary conditions: either immediately after the document is signed and the necessary initials are provided or when your primary physician determines that you are unable to make your own health care decisions. The choice is yours, and you must clearly indicate your preference on the form. This ensures that the transition of decision-making power is in line with your expectations and circumstances.
Can I revoke or change my Advance Health Care Directive?
Yes, you have the full right to revoke or replace your Advance Health Care Directive at any time. Life circumstances and relationships change, and your health care directive can reflect those changes. Whether you wish to appoint a different agent, modify your health care instructions, or cancel the directive altogether, you can do so. It's recommended to communicate any changes to your health care agent, family, and health care providers to ensure that everyone is aware of your current wishes.
Common mistakes
When filling out the 3-1 Health Care Directive form, people often make mistakes that can affect the clarity and effectiveness of their health care wishes. It's essential to approach this document with attention to detail to ensure your preferences are understood and followed. Below are five common mistakes:
-
Not discussing the directive with the chosen agent. It's crucial that the person you designate as your agent fully understands your wishes and is willing to take on the responsibility. Failing to have this conversation can lead to confusion and hesitancy should they need to make decisions on your behalf.
-
Using vague language in Part 2 of the form. When specifying your health care instructions, clarity is key. Ambiguous statements can lead to interpretation issues and may result in care that doesn't align with your wishes.
-
Omitting to initial choices in the End of Life Decisions or Donation of Organs at Death sections. The form requires your initials next to your choices to validate them. Skipping this step can make your selections nonbinding.
-
Forgetting to add contact information for alternate agents. Naming a primary agent is a crucial step, but providing details for alternate agents ensures there is no delay in decision-making if your first choice cannot serve.
-
Neglecting to update the document. Life changes, such as a change in health status or a shift in personal relationships, may affect your decisions. Regular reviews and updates to your directive ensure it always reflects your current wishes.
By avoiding these common errors, you can create a comprehensive and clear Health Care Directive that accurately reflects your health care preferences.
Documents used along the form
In preparing for health care decisions, especially those that need to be made when one might not be able to make them independently, the FORM 3 - 1 Advance Health Care Directive plays a crucial role. However, it’s important to know that this form is often one piece of a broader set of documents that individuals and families should consider to ensure comprehensive planning. These documents, each serving a unique purpose, work together to fully communicate a person's wishes regarding health care, end-of-life decisions, and beyond.
- Living Will: This document complements the health care directive by allowing individuals to outline their preferences for medical treatment and life-sustaining measures in more detail. It becomes relevant when a person is terminally ill or in a permanent vegetative state and unable to communicate their wishes.
- Durable Power of Attorney for Health Care: Although the Advance Health Care Directive includes a section for designating a health care agent, a standalone Durable Power of Attorney for Health Care provides an alternative form. It strictly focuses on appointing someone to make health care decisions, ensuring there's someone with legal authority to act according to the individual's wishes if they're unable to do so themselves.
- Physician Orders for Life-Sustaining Treatment (POLST): This form is designed for those already suffering from a serious illness. It goes beyond the Advance Directive by turning an individual's wishes regarding life-sustaining treatments into medical orders. This ensures that health care providers know and are legally required to follow these instructions.
- Will and Testament: While not directly related to health care decisions, a will is essential for articulating how one's property and affairs should be handled after death. Including a will in one’s planning can ease the administrative and emotional burdens on families during a difficult time.
Each of these documents serves a specific purpose and, together with the FORM 3 - 1 Advance Health Care Directive, forms a comprehensive plan that respects an individual's wishes regarding health care and beyond. Consultation with legal professionals can help ensure these documents are properly executed and reflect the person's desires accurately.
Similar forms
Living Will: Much like the Advance Health Care Directive Form, a living will is a document where individuals can specify their wishes regarding medical treatment in situations where they're unable to communicate or make decisions for themselves. Both documents allow for preferences to be laid out regarding the withholding or withdrawal of life-sustaining procedures.
Durable Power of Attorney for Healthcare: This document is similar to the designating of an agent aspect in the Advance Health Care Directive. It lets individuals appoint someone else to make healthcare decisions on their behalf if they become incapacitated or unable to express their wishes, covering a wide range of decisions except those specifically restricted.
Do Not Resuscitate (DNR) Order: A DNR is a type of advance directive that focuses specifically on the refusal of cardiopulmonary resuscitation (CPR) if the individual's heart stops or if they stop breathing. While more specific than an Advance Health Care Directive, both documents guide healthcare professionals on how to proceed with treatment in critical situations.
Organ and Tissue Donation Registration: Similar to Part 3 of the Advance Health Care Directive, which deals with donations of organs and tissues at death, this document allows individuals to express their wishes regarding organ and tissue donation. However, while organ and tissue donation registration often happens through state registries, the Advance Health Care Directive includes these wishes within a broader document that also addresses other healthcare decisions.
Physician Orders for Life-Sustaining Treatment (POLST): A POLST form complements an Advance Health Care Directive by transforming an individual's treatment preferences into medical orders. While an Advance Health Care Directive is more comprehensive in scope, a POLST is used to ensure that healthcare providers are aware of and honor the patient's specific wishes regarding life-sustaining treatments in emergency situations.
Dos and Don'ts
Completing the 3-1 Health Care Directive form is a significant step in ensuring that your health care preferences are known and respected. To assist in this process, here are four essential dos and don'ts to keep in mind:
Do:
- Discuss your wishes with the person you intend to name as your agent before you fill out the form. It's crucial that they understand your preferences and are willing to act on your behalf.
- Be as specific as possible in Part 2 of the form if you have definite preferences about your health care. This clarity can guide your agent and health care providers in making decisions that align with your values and wishes.
- Include contact information for your agent and any alternate agents. Make sure the addresses and phone numbers are current and accurate to ensure they can be reached if needed.
- Sign and date the form in the presence of two qualified witnesses or a notary public, as required by your state's laws. This step is essential to make the directive legally binding.
Don't:
- Select an agent who is an operator or employee of a community care or residential care facility where you are receiving care, or your supervising health care provider, unless they are related to you by blood, marriage, or are a coworker. This conflict of interest could affect the impartiality of your health care decisions.
- Leave sections blank if you have specific wishes. If you do not fill out parts of the form, it may be assumed that you are indifferent to those decisions or wish for your agent to choose for you, which might not reflect your actual desires.
- Forget to provide a copy of the signed directive to your physician, health care institution, and any other health care providers you may have. They need to have this document on file to follow your health care instructions.
- Assume that once completed, the directive cannot be changed. Your health care preferences might evolve over time, so review and update your directive as necessary, ensuring it always reflects your current wishes.
Misconceptions
There are several common misconceptions about the Form 3-1 Advanced Health Care Directive that individuals often encounter. The purpose of a detailed analysis is to clarify these misunderstandings and provide accurate information for those considering or using this form for their health care planning.
Misconception 1: The directive only applies to end-of-life decisions. While the directive does cover decisions related to the end of life, it also encompasses a broader range of health care decisions, such as the specific types of medical care or treatments one prefers, including decisions about artificial nutrition and hydration.
Misconception 2: Only the elderly or terminally ill need to complete it. People of all ages can benefit from having an advanced health care directive. Unexpected critical medical situations can arise at any age, and having a directive helps ensure that an individual’s health care preferences are known and considered.
Misconception 3: You cannot change your agent once the document is signed. The document can be updated or revoked at any time by the person who created it, allowing for the appointment of a new health care agent if the individual's circumstances or preferences change.
Misconception 4: Completing the form means giving up control over your health decisions. The purpose of the directive is precisely the opposite; it is a tool for individuals to express their wishes and maintain control over their health care decisions, even if they become unable to communicate their wishes directly.
Misconception 5: The health care agent can make decisions before the individual is incapacitated. The agent’s authority to make decisions is typically activated only when the principal’s primary physician certifies that the principal is unable to make their own health care decisions, unless the directive specifies otherwise.
Misconception 6: The form automatically includes decisions about organ donation. Organ donation preferences are an optional part of the form. Individuals have the choice to include instructions about organ donation, and they can specify which organs they wish to donate and for what purposes.
Misconception 7: The directive enables the agent to manage the individual's financial affairs. The directive is strictly limited to health care decisions. The management of finances or property would require a different type of legal document, such as a durable power of attorney for finances.
Misconception 8: The document is too complicated and requires a lawyer to fill out. While it’s always advisable to consult with legal counsel for comprehensive estate planning, the Form 3-1 Advanced Health Care Directive is designed to be completed by individuals without the need for a lawyer. Clear instructions are included with the form to guide individuals through the process.
Understanding these key points about the Form 3-1 Advanced Health Care Directive can help individuals make informed decisions about their health care planning, ultimately ensuring their wishes are respected during critical health care situations.
Key takeaways
Filling out and effectively using the Form 3-1 Advance Health Care Directive is a critical step in managing your health care preferences. Here are seven key takeaways to guide you through this important process:
- Appointment of an Agent: You can appoint someone you trust to make health care decisions on your behalf if you become unable to do so. This form allows not only for a primary agent but also for alternate agents in case the primary is not available.
- Authority of the Agent: The agent you appoint is granted extensive authority to manage your health care, including decisions on treatments, health care providers, and end-of-life care, except in areas you specifically limit.
- Effective Timing: You have the option to specify when your agent’s authority becomes effective—either immediately or only when you are determined to be unable to make your own health care decisions.
- Personal Wishes and Instructions: The directive allows you to provide specific instructions about your health care preferences, especially regarding end-of-life decisions and pain relief, ensuring your wishes are followed as closely as possible.
- Post-Death Decisions: You can authorize your agent to donate your organs, authorize an autopsy, and direct the disposition of your remains, with the option to specify or restrict the types of donations and uses.
- Optional Donation Specifications: If choosing to donate organs or tissues, you can specify the purposes for which they can be used, such as transplant, research, therapy, or education, and set boundaries regarding the use of your donated tissues.
- Revocation and Updates: The directive is not set in stone. It can be revoked or replaced at any time, allowing you to update your document as your health or preferences change.
It is crucial to discuss your health care directive with the appointed agent to ensure they understand and are willing to follow your preferences. Completing the Form 3-1 Advance Health Care Directive is a proactive step in managing your future health care needs and ensuring your wishes are known and respected.
Popular PDF Forms
Employee Corrective Action Examples - Optimizes the process of employee assessment and correction, reinforcing desired performance standards.
Incident Report Construction - Facilitates a proactive approach to construction safety, with fields for detailing preventive actions taken post-incident.
Ysq-r - Guides individuals through self-exploration of trust issues and self-protection mechanisms.