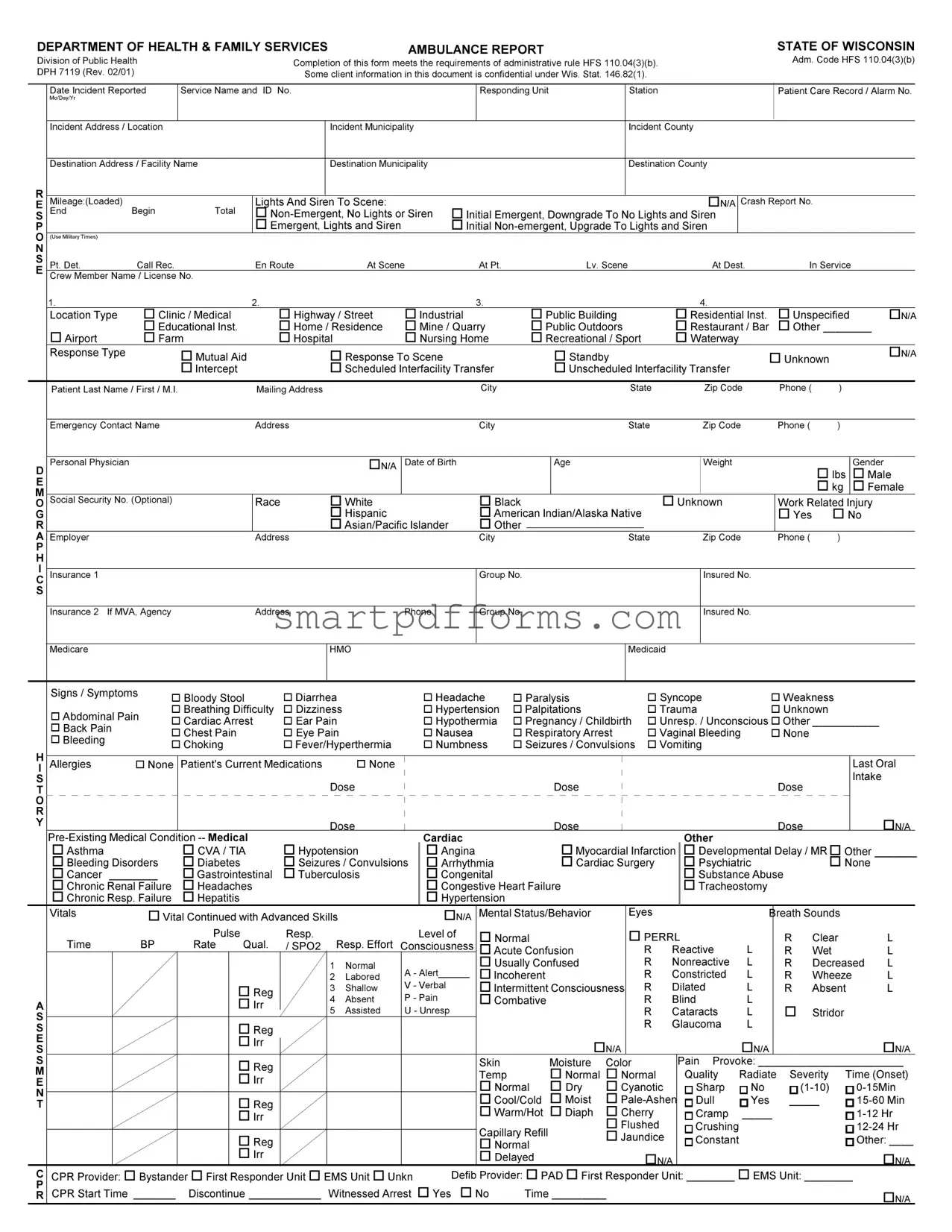
Blank Ambulance Report PDF Template
In the earnest endeavor to streamline emergency medical services and bolster patient care coordination, the Ambulance Report Form, as endorsed by the Department of Health & Family Services in the State of Wisconsin, emerges as a pivotal document stirring the dimensions of pre-hospital medical records. Serving the directives stipulated under administrative rule HFS 110.04(3)(b), this comprehensive form embarks on capturing a substantial variety of details, starting from the incident's nuts and bolts – including the date, location, responding unit particulars, patient's demographic and medical history – to the nuanced clinical evaluations and the administered pre-hospital emergency care interventions. The format also thoughtfully incorporates sections addressing the patient's insurance information, medical alerts like allergies and pre-existing conditions, as well as meticulously tracking the patient's journey from the incident scene to the ultimate healthcare destination, outlining the urgency and nature of the response throughout. Privacy considerations are deftly handled, acknowledging the sensitive nature of client information under Wis. Stat. 146.82(1), thus ensuring a balanced approach between comprehensive record-keeping and respect for patient confidentiality.
Preview - Ambulance Report Form
DEPARTMENT OF HEALTH & FAMILY SERVICES |
AMBULANCEREPORT |
|
|
STATE OF WISCONSIN |
||||||||
|
|
|
|
|
|
|
|
|
|
|||
Division of Public Health |
|
|
Completion of this form meets the requirements of administrative rule HFS 110.04(3)(b). |
|
Adm. Code HFS 110.04(3)(b) |
|||||||
|
|
|
|
|
|
|
||||||
DPH 7119 (Rev. 02/01) |
|
|
Some client information in this document is confidential under Wis. Stat. 146.82(1). |
|
|
|||||||
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||
|
Date Incident Reported |
Service Name and ID No. |
|
|
RespondingUnit |
Station |
|
Patient Care Record / Alarm No. |
||||
|
Mo/Day/Yr |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Incident Address / Location |
|
|
|
|
Incident Municipality |
|
|
Incident County |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Destination Address / Facility Name |
|
|
|
Destination Municipality |
|
|
Destination County |
|
|
||
R |
|
|
|
|
|
|
|
|
|
|
|
|
E |
Mileage:(Loaded) |
|
|
|
Lights And Siren To Scene: |
|
|
|
οN/A |
Crash Report No. |
||
S |
End |
Begin |
|
Total |
οInitial Emergent, Downgrade To No Lights and Siren |
|
||||||
P |
|
|
|
|
οEmergent,Lights and Siren |
|
|
|||||
O(UseMilitaryTimes)
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
Pt. Det. |
CallRec. |
En Route |
At Scene |
At Pt. |
|
Lv. Scene |
|
At Dest. |
|
In Service |
|
||||||
E |
|
|
|
|
||||||||||||||
Crew Member Name / License No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
1. |
|
2. |
|
|
3. |
|
|
|
|
4. |
|
|
|
|
|
|
|
|
LocationType |
οClinic / Medical |
οHighway / Street |
οIndustrial |
|
οPublic Building |
οResidentialInst. |
|
οUnspecified |
οN/A |
|||||||
|
|
|
οEducationalInst. |
οHome / Residence |
οMine / Quarry |
οPublicOutdoors |
οRestaurant / Bar |
|
οOther ________ |
|||||||||
|
|
οAirport |
οFarm |
οHospital |
οNursing Home |
οRecreational/Sport |
οWaterway |
|
|
|
|
|
||||||
|
|
Response Type |
οMutual Aid |
|
οResponse To Scene |
|
|
οStandby |
|
|
οUnknown |
οN/A |
||||||
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
οIntercept |
|
οScheduledInterfacilityTransfer |
|
οUnscheduledInterfacilityTransfer |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Last Name / First / M.I. |
Mailing Address |
|
|
City |
|
|
State |
|
Zip Code |
|
Phone ( |
) |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Emergency Contact Name |
Address |
|
|
City |
|
|
State |
|
Zip Code |
|
Phone ( |
) |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D |
Personal Physician |
|
|
οN/A |
Date of Birth |
|
|
Age |
|
Weight |
|
|
|
|
Gender |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ο lbs |
|
οMale |
||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οkg |
|
οFemale |
|
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
O |
Social Security No. (Optional) |
Race |
οWhite |
|
οBlack |
|
|
|
|
οUnknown |
|
WorkRelatedInjury |
||||||
G |
|
|
|
οHispanic |
|
οAmericanIndian/AlaskaNative |
|
|
|
ο Yes |
ο No |
|||||||
R |
|
|
|
οAsian/PacificIslander |
οOther |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
A Employer |
|
Address |
|
|
City |
|
|
State |
|
Zip Code |
|
Phone ( |
) |
|
|
|||
P |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurance 1 |
|
|
|
|
Group No. |
|
|
|
|
|
Insured No. |
|
|
|
|
|
||
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurance 2 If MVA, Agency |
Address |
|
Phone |
Group No. |
|
|
|
|
|
Insured No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medicare |
|
|
HMO |
|
|
|
|
Medicaid |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signs / Symptoms
οAbdominal Pain
οBack Pain
οBleeding
ο Bloody Stool |
ο Diarrhea |
ο Headache |
ο Paralysis |
ο Syncope |
ο Weakness |
ο BreathingDifficulty |
ο Dizziness |
ο Hypertension |
ο Palpitations |
ο Trauma |
ο Unknown |
ο CardiacArrest |
ο Ear Pain |
ο Hypothermia |
ο Pregnancy / Childbirth |
ο Unresp./Unconsciousο Other___________ |
|
ο Chest Pain |
ο Eye Pain |
ο Nausea |
ο Respiratory Arrest |
ο VaginalBleeding |
ο None |
ο Choking |
ο Fever/Hyperthermia |
ο Numbness |
ο Seizures / Convulsions |
ο Vomiting |
|
H |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Allergies |
|
|
|
|
|
ο None |
Patient's Current Medications |
|
|
|
ο None |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LastOral |
||||||||||||||||||||||||||||||||||||||||||||||||||||
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dose |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dose |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dose |
|
|
|
|
|
|
|
|
Intake |
|
|
||||||||||||||||||||||
T |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Y |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dose |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dose |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dose |
|
|
|
|
|
|
|
|
|
οN/A |
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cardiac |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
οAsthma |
|
|
|
|
|
|
|
|
|
|
|
|
οCVA / TIA |
|
|
|
|
|
οHypotension |
|
|
|
|
|
οAngina |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οMyocardial Infarction |
|
οDevelopmental Delay / MRοOther _______ |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
οBleedingDisorders |
οDiabetes |
|
|
|
|
|
οSeizures / Convulsions |
|
|
ο Arrhythmia |
|
|
|
|
|
|
|
|
|
οCardiac Surgery |
|
|
|
ο Psychiatric |
|
|
|
|
|
|
|
|
οNone |
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
οCancer |
________ |
|
|
|
οGastrointestinal |
οTuberculosis |
|
|
|
|
|
οCongenital |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οSubstance Abuse |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
οChronic Renal Failure |
οHeadaches |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οCongestiveHeartFailure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οTracheostomy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
οChronic Resp. Failure |
οHepatitis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οHypertension |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|
Vitals |
|
|
|
|
|
|
|
οVital Continued with Advanced Skills |
|
|
|
|
|
|
|
|
οN/A |
MentalStatus/Behavior |
|
|
|
|
|
|
Eyes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BreathSounds |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pulse |
|
|
|
|
|
|
Resp. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Levelof |
οNormal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οPERRL |
|
|
|
|
|
|
|
|
|
R |
|
Clear |
|
L |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
Time |
|
|
|
|
|
|
BP |
|
|
Rate |
|
|
Qual. |
|
/ SPO2 |
|
|
|
Resp.Effort |
|
Consciousness |
οAcuteConfusion |
|
|
|
|
|
|
|
|
R |
|
Reactive |
|
L |
|
|
|
R |
|
Wet |
|
L |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
Normal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οUsually Confused |
|
|
|
|
|
|
|
|
R |
|
Nonreactive |
|
L |
|
|
|
R |
|
Decreased |
L |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
Labored |
|
A - Alert______ |
οIncoherent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
Constricted |
|
L |
|
|
|
R |
|
Wheeze |
|
L |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οReg |
|
|
|
|
|
|
|
|
3 |
|
Shallow |
|
V - Verbal |
οIntermittentConsciousness |
|
|
R |
|
Dilated |
|
L |
|
|
|
R |
|
Absent |
|
L |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
Absent |
|
P - Pain |
οCombative |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
Blind |
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οIrr |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
Assisted |
|
U - Unresp |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
Cataracts |
|
L |
|
|
|
ο |
|
Stridor |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
Glaucoma |
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οReg |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οIrr |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οN/A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οN/A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οN/A |
|
||||||||||||||||||
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οReg |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Skin |
|
|
|
|
|
|
|
Moisture |
|
|
Color |
|
|
Pain Provoke:________________________ |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Temp |
|
|
|
|
|
|
|
οNormal οNormal |
|
|
|
Quality |
Radiate |
|
|
Severity Time(Onset) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οIrr |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οNormal |
ο Dry |
|
|
οCyanotic |
|
|
|
|
|
Sharp |
|
No |
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οReg |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οCool/Cold |
ο Moist |
|
|
|
|
|
Dull |
|
|
Yes |
_____ |
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
T |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οWarm/Hot |
οDiaph |
|
|
οCherry |
|
|
|
|
|
Cramp |
_____ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οIrr |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οFlushed |
|
|
|
|
|
Crushing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CapillaryRefill |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ο |
Reg |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οJaundice |
|
|
|
|
|
Constant |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other:____ |
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οNormal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οIrr |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οDelayed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οN/A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οN/A |
||||||||||||||||||||||||
C CPR Provider: οBystander οFirst Responder Unit οEMS Unit οUnkn |
|
|
|
|
|
|
Defib Provider: οPADοFirst Responder Unit: ________οEMS Unit: ________ |
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
P |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Discontinue ____________ Witnessed Arrest οYes οNo |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
R CPR Start Time _______ |
|
|
|
Time _________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οN/A |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
DEPARTMENT OF HEALTH & FAMILY SERVICES |
AMBULANCEREPORT |
STATE OF WISCONSIN |
||
|
|
|
||
Division of Public Health |
Completion of this form meets the requirements of administrative rule HFS 110.04(3)(b). |
page 2 |
||
|
|
|||
DPH 7119 (Rev. 02/01) |
Some client information in this document is confidential under Wis. Stat. 146.82(1). |
|
||
|
|
|
|
|
Service Name and ID No. |
|
|
Patient Last Name / First / M.I. |
Patient Care Record / Alarm No. |
|
|
|
|
|
Physical Examination
P
H
Y
SI Injury / Pain Location
CHead / Face
A
LNeck
EChest / Axilla
AX Abdomen
MBack / Flank
I
N Pelvis / Hip
A |
L Arm |
U |
L |
J |
T |
||||
I |
R Arm |
U |
L |
J |
O |
|
|
|
|
N |
L Leg |
U |
L |
J |
|
R Leg |
U |
L |
J |
|
|
|
|
|
|
/Abrasion |
|
Swe |
|
|
Pain |
|
|
Dis |
|
GunshotLacerationPunctureSoft |
|
|
lling |
||
B |
|
|
Burn |
______________ |
||||||
|
(No |
Trauma) |
|
|
/Stab |
|
|
|||
|
|
|
FX |
|
issue |
|
|
|||
|
|
lunt |
/ |
|
|
T |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οN/A Glasgow Coma Scale |
|
|
|
|
A. |
Eye Opening |
SceneEnroute |
|
|
|
Spontaneous |
4 |
4 |
|
|
Tovoice |
3 |
3 |
Time |
|
To pain |
2 |
2 |
|
|
|
|||
|
None |
1 |
1 |
|
B. |
VerbalResponse |
|
|
|
|
|
|
||
|
Oriented |
5 |
5 |
|
|
Confused |
4 |
4 |
|
|
Inappropriatewords |
3 |
3 |
|
|
IncomprehensibleWords |
2 |
2 |
|
|
None |
1 |
1 |
|
C. |
MotorResponse |
|
|
|
|
Obeys commands |
6 |
6 |
|
|
Purposefulmovement |
5 |
5 |
|
|
Withdrawstopain |
4 |
4 |
|
|
Flexiontopain |
3 |
3 |
|
|
Extensiontopain |
2 |
2 |
|
|
None |
1 |
1 |
|
A. + B. + C. = |
_____ |
____ |
ο |
|
|
|
|
|
N/A |
T |
MotorVehicleCrash |
|
|
|
|
οN/A |
|
Type |
|
οN/A |
ExteriorDamageοN/A |
InteriorDamage οN/A |
|
Restraints |
|
οN/A |
SafetyEquipment |
οN/A |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
R |
|
|
|
|
|
|
|
|
|
ο Car |
ο Motorcycle |
οNone |
|
οNone |
|
|
|
|
|
Obs |
Rprt |
|
|
|
|
||||
A |
|
|
|
|
|
|
|
|
|
|
|
|
Airbag |
|
ο |
ο |
|
οNone |
οFloat. Dev. |
||||||||||
|
|
|
|
|
|
|
|
|
οTruckο ATV |
|
ο Minor |
|
οSpideredWindow |
|
|
|
|||||||||||||
U |
|
earR |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
M |
|
|
|
|
|
|
|
|
ο Van ο Snowmobile |
οModerate |
|
οSt. Wh. Bent |
|
LapBelt |
ο |
ο |
|
οHelmet |
οUnknown |
||||||||||
A |
|
|
|
|
|
|
|
|
|
ο Semi οWatercraft |
ο Major |
|
οCompart.Intrusion |
|
ShoulderBelt |
ο |
ο |
|
ο Eye Prot. |
|
|||||||||
T |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
I |
|
|
|
|
|
|
|
|
|
ο Bus |
οAircraft |
|
οRollover |
|
οPatient Ejected |
|
ChildSeat |
ο |
ο |
|
οProt.Clothing |
|
|||||||
C P = Patient Location in Vehicle |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
X = Location of Damage to Vehicle |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
I |
CauseofInjury |
οN/A οChemical Exposure |
|
οExcessive Heat |
οLightning |
|
|
|
ο Physical Assault |
οStings (Plant / Animal) |
|||||||||||||||||||
N |
οAircraftRelated |
|
|
οChildBatteringSuspected |
ο Fall |
|
|
ο Machinery Injury |
|
οPoison, Not Drugs |
οWaterTransportIncident |
||||||||||||||||||
J |
|
|
οDrowning |
|
|
οFire / Flames |
οMechanicalSuffocation |
|
οRadiationExposure |
οUnknown |
|
||||||||||||||||||
U |
οAthletic Event |
|
|
|
οDrugIngestion |
|
οMotor Vehicle |
οSexual Assault |
|
|
οOther___________ |
||||||||||||||||||
R |
ο Bicycle Crash |
|
|
|
οFirearm Accidental |
οMotor Vehicle (Traffic) |
|
οSmokeInhalation |
|
|
|
||||||||||||||||||
Y |
ο Bite |
|
|
|
οExcessive Cold |
|
οFirearm Assault |
οPedestrianTraffic |
|
οStabbing |
|
|
|
|
|
||||||||||||||
|
|
ProviderImpression If more than one impression is checked, Circle Primary One |
οHypothermia |
|
οRespiratory Arrest |
οSyncope / Fainting |
|||||||||||||||||||||||
|
|
οHypovolemia / Shock |
|
οRespiratory Distress |
οTraumatic Injury |
||||||||||||||||||||||||
|
|
οAbd. Pn. / Problems |
οCardiac Arrest |
|
οElectrocution |
οIntoxicationSuspected/ |
|
οSeizure |
|
|
|
οVaginalHemorrhage |
|||||||||||||||||
|
|
οAirway Obstruction οCardiac Rhythm. Disturb. |
οGI Bleed |
|
|
AlcoholIngestion |
|
ο |
Sexual Assault / Rape |
ο |
Unknown |
|
|||||||||||||||||
|
|
οAllergic Reaction |
|
οChest Pn. Discomfort |
|
οHeadache |
|
οObviousDeath |
|
οToxicInhalation |
|
|
ο Other___________ |
||||||||||||||||
|
|
οAlteredL.O.C. |
|
|
οCongestiveHeartFailure |
οHypertension |
οPoison / Drug Ingestion |
|
οStings / Bites |
|
|
|
|
|
|||||||||||||||
|
|
οBehavioral / Psych |
οDiabetic Symptoms |
|
οHyperthermia / Fever |
οPregnancy / Ob Delivery |
οStroke / CVA / TIA |
|
|
|
|||||||||||||||||||
|
|
Chief Complaint / Mechanism of Injury: |
|
|
|
|
|
|
|
Time of Onset: |
|
ProcedureorTreatment |
|
EMT |
EMT |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οAssistedVentilation |
|
_____ |
_____ |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οBackboard |
|
|
|
_____ |
_____ |
||
|
|
Comments: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οBleedingControl |
|
_____ |
_____ |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οBurn Care |
|
|
|
_____ |
_____ |
||||
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ο CPR |
|
|
|
|
_____ |
_____ |
|||
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οCervicalImmobilization |
|
_____ |
_____ |
||||||
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οDNR Protocol |
|
|
|
_____ |
_____ |
||||
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οGlucoseAdministration |
|
_____ |
_____ |
||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οNasopharyngeal Airway |
|
_____ |
_____ |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οObstetric Care / Delivery |
_____ |
_____ |
||||||
T |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οOropharyngeal Airway |
|
_____ |
_____ |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οO2 By Mask ______ liters |
_____ |
_____ |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οO2 By Cannula ______ liters |
_____ |
_____ |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ο Physical Exam |
|
|
|
_____ |
_____ |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οRadio / Phone Report |
|
_____ |
_____ |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οSplint of Extremity |
|
_____ |
_____ |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οTractionSplint |
|
|
|
_____ |
_____ |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οVital Signs |
|
|
|
_____ |
_____ |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οOTHER:________________ |
_____ |
_____ |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οNone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If an advanced skill is performed,completeformDPH7300 |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
IncidentDisposition |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LightsAndSirenDuringTransport: |
οN/A |
||||||||
|
|
οTreated / Transported by EMS |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
DestinationType |
- AND - DestinationDetermination |
οTreated/TransferredCare |
|
οNo Treat. Needed |
|
||||||||||||||||||||||
|
|
|
οEmergent, LightsandSiren |
|
|
||||||||||||||||||||||||
|
|
οHome / Residence |
|
|
οClosest Facility |
|
οTo |
|
|
|
|
|
οInitial Emergent, Downgrade To No Lights and Siren |
||||||||||||||||
M |
οPolice / Jail |
|
|
|
οDiversion |
|
|
οTo ALS Unit |
|
|
οDead at Scene |
|
|||||||||||||||||
οMedical Office / Clinic |
|
οEMT Choice |
|
|
οTo BLS Unit |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
I |
οSkilled Nursing Facil. |
|
οLaw Enforce. Choice |
|
οTo Law Enforcement |
|
οCancelled |
|
PatientTransported |
|
|
OtherServicesonScene |
|||||||||||||||||
S |
οHospital Direct Admit |
|
οManaged Care |
|
|
|
|
|
|
|
|
|
|
οProne |
|
|
|
οLawEnforcement______ |
|||||||||||
C |
οHospital ED |
|
|
|
οOn Line Med. Direction |
|
οTreated / No Transport |
|
οUnknown |
|
οSupine |
|
|
|
οFire _______ |
||||||||||||||
EL |
ο Morgue |
|
|
|
οPatient / Family Choice |
|
οTreat. / Trans. by Priv. Veh. |
|
|
|
|
|
οSitting |
|
|
|
οOther___________ |
||||||||||||
L |
ο Other |
|
|
|
οPatient / Phys. Choice |
|
οTreat. / Trans. by Other Means |
|
οNo Patient Found |
|
οPatientRestrained |
οNone |
|
||||||||||||||||
A |
|
|
|
|
|
οProtocol |
|
|
οTreated and Released |
|
|
|
|
|
οHead Elevated |
|
|
ο Physician |
|
||||||||||
|
|
|
|
|
οSpecialty Center |
|
|
|
|
|
|
|
|
|
|||||||||||||||
N |
|
|
|
|
|
|
ο |
Patient Refused Care |
|
|
|
|
|
οFeetElevated |
|
|
οFirstResponder_______ |
||||||||||||
|
|
|
|
|
ο Other |
|
|
|
|
|
|
|
|
|
|
||||||||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οIn_____LateralPosition οNurse / PhysicianAssistant |
||||||||||||
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οOther___________ |
|
|
οN/A |
||||||
U |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
S |
ArrivalStatusοN/A |
PPE Used οN/A |
|
Facility Notified By |
οN/A |
DifficultiesEncountered |
Time Report Received: By: |
|
|
|
|
|
|
||||||||||||||||
|
|
οUnchanged |
|
οGloves |
|
οRadio |
|
|
|
|
οDispatch οOther _____ |
Report Given To: ______________________________________ |
οN/A |
||||||||||||||||
|
|
οBetter |
|
ο Gown |
|
οPhone |
|
|
|
οExtrication |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
οWorse |
|
οGoggles |
|
οUnable* |
|
|
|
οHazardousMaterial |
EMT Signature |
|
|
|
|
|
|
|
|
||||||||||
|
|
οDOA |
|
ο Mask |
|
οNo Need* |
|
|
|
οLanguageBarrier |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
οUnknown |
|
οOther________ |
|
οDirect |
|
|
|
|
οRoad |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
οEKG Telemetry |
|
|
οUnsafe Scene |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
*Explain________________ |
οVehicle Problems |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
οWeather |
|
οN/A |
|
|
|
|
|
|
|
|
|
|
|
Form Data
| Fact Name | Detail |
|---|---|
| Governing Law | Completion of this form meets the requirements of administrative rule HFS 110.04(3)(b) under Wisconsin Administrative Code. |
| Confidentiality | Some client information in this document is confidential under Wisconsin Statute 146.82(1). |
| Form Identification | The form is identified as DPH 7119, last revised in February 2001. |
| Usage | The form is used by emergency services in the State of Wisconsin to report ambulance services provided. |
| Required Information | It collects detailed information, including date, service name, incident location, patient care record number, and details of the emergency response. |
| Patient Information | Includes patient name, contact details, insurance information, treatment administered, and transport details. |
| Medical Condition and Treatment | Documents signs/symptoms, allergies, current medications, pre-existing medical conditions, and procedures or treatments performed. |
| Incident and Disposition | Covers details of the incident, such as cause of injury, response type, vehicle information for crashes, provider impressions, and the patient's disposition. |
Instructions on Utilizing Ambulance Report
Filling out the Ambulance Report form is a process that ensures all critical details of the ambulance service provided during an emergency are accurately documented. This information is pivotal for several reasons, including medical follow-up, administrative needs, and legal considerations. Accurately completing this form not only facilitates seamless patient care but also complies with the administrative rules laid out by the Department of Health & Family Services. Here are the steps to properly fill out the form:
- Start by entering the date the incident was reported in the "Date Incident Reported" section.
- Fill in the "Service Name and ID No." followed by the "Responding Unit Station."
- Enter the "Patient Care Record / Alarm No." to link this report to the patient's ongoing medical records.
- Document the incident location, including "Incident Address / Location," "Incident Municipality," and "Incident County."
- Provide details of the destination including "Destination Address / Facility Name," "Destination Municipality," and "Destination County."
- In the section for "Mileage," fill in the "Begin" and "End" odometer readings to calculate the "Total" miles traveled.
- Indicate the use of "Lights And Siren To Scene" by selecting the appropriate option.
- Record the chronology under the "Pt. Det.," noting the times for "Call Rec.," "En Route," "At Scene," "At Pt. Lv. Scene," "At Dest.," and "In Service."
- List all crew members involved, including their "Name" and "License No."
- Specify the "Location Type" and "Response Type" by selecting the appropriate options.
- Enter patient information under the "Patient" section, including their "Last Name, First Name, M.I.," "Mailing Address," "City, State, Zip Code," "Phone," "Emergency Contact Name," and contact details.
- Select the "Personal Physician" option if applicable or mark it as "N/A."
- Fill in the patient's "Date of Birth," "Age," "Weight," and "Gender."
- Optionally include the "Social Security No.," and select the patient's "Race."
- If the incident was work-related, mark "Yes" or "No," and fill in the employer's information.
- Complete the "Insurance" section with relevant details about the patient's insurance coverage.
- Tick the appropriate boxes under "Signs / Symptoms," "Allergies," and "Patient's Current Medications."
- Document any pre-existing medical conditions the patient has.
- Record the patient's initial vitals in the "Vitals" section.
- If CPR or defibrillation was provided, include details in the designated areas.
- For the physical examination, note all findings, including the "Glasgow Coma Scale" and details of any injuries.
- Document the incident details, such as cause of injury, provider impression, and chief complaint.
- Describe any procedures or treatments provided, marking the appropriate boxes and including comments as necessary.
- Complete the "Incident Disposition" section with information about patient transport and destination determination.
- List other services on scene, and select the patient's position during transport.
- Fill in the section on "Arrival Status," "PPE Used," and how the "Facility Notified By."
- Note any "Difficulties Encountered" during the course of the service.
- Ensure the EMT signs at the bottom of the form, indicating the completion and verification of the reported information.
After the form is fully completed, it must be reviewed for accuracy, then submitted to the appropriate medical facility or administrative office as required. This step ensures that the patient's care continues smoothly and that all relevant parties have the necessary information. Remember, the timely and accurate completion of the Ambulance Report form is critical in maintaining the integrity of patient care and legal compliance.
Obtain Answers on Ambulance Report
What is the purpose of the Ambulance Report form?
The Ambulance Report form, designed by the State of Wisconsin's Department of Health & Family Services, serves a critical role in documenting the details of patient care and transport by emergency services. By meticulously recording incident and patient information, response details, and treatment provided en route to a medical facility, this form satisfies the requirements set forth under administrative rule HFS 110.04(3)(b). The comprehensive capture of such data is essential not only for ensuring continuity of care but also for legal, administrative, and quality improvement purposes.
Is the information provided on the Ambulance Report form confidential?
Yes, patient information documented on the Ambulance Report form is considered confidential, as protected under Wisconsin Statute 146.82(1). This statute imposes strict limitations on the disclosure of health information, ensuring that sensitive patient data is shared only among authorized individuals and entities, thereby safeguarding patient privacy.
Who completes the Ambulance Report form?
Crew members aboard the ambulance, including EMTs (Emergency Medical Technicians) and paramedics, are responsible for filling out the form. Each member contributes by documenting specific observations and actions taken during patient care, from the initial response through transport to the eventual handover at the destination facility. Their input is vital for a complete and accurate record of the incident and patient care provided.
What type of information is recorded on the Ambulance Report form?
The Ambulance Report form captures a wide array of essential information. This includes:
- Details of the incident, such as location, time, and nature of the call
- Patient's personal and insurance information
- Medical history, signs, symptoms, and pre-existing conditions of the patient
- Details of the response, including transportation and treatment administered
- Crew member identification and participation
- Patient's condition upon handover and the destination facility specifics
This spectrum of data plays a crucial role in clinical decision-making, billing processes, and legal documentation.
How does the Ambulance Report form impact patient care?
By providing a detailed account of the pre-hospital care and condition of the patient, the Ambulance Report form ensures a smoother transition and continuity of care upon arrival at a medical facility. It equips the receiving healthcare professionals with the information necessary to make informed decisions regarding further treatment. The documentation also assists in identifying areas for improvement in emergency medical services and patient care protocols.
Can the information on the Ambulance Report form be used for legal purposes?
Yes, the Ambulance Report form can serve as a vital piece of evidence in legal cases. It provides an official record of the patient's condition at the scene, the care provided by emergency responders, and the circumstances surrounding the incident. This information can be crucial in personal injury lawsuits, insurance claims, and investigations into the incident.
Are there protocols for amending or correcting information on the Ambulance Report form?
Yes, while the exact process may vary by jurisdiction, generally, there are established procedures for amending or correcting information on the Ambulance Report form. Any amendments must be made carefully to preserve the integrity of the original document while ensuring the accuracy of the patient record. Typically, corrections are clearly marked, dated, and signed by the individual making the amendment.
How is the Ambulance Report form submitted and stored?
Upon completion, the Ambulance Report form is submitted to the receiving medical facility along with the patient. Copies may also be retained by the EMS provider for their records. The form is typically stored in both physical and electronic formats, ensuring it can be readily accessed for patient care, review, or legal purposes while maintaining compliance with confidentiality laws and regulations regarding health information.
Common mistakes
Completing an Ambulance Report form is a critical step in ensuring that patients receive appropriate care and that their medical records are accurately documented. However, mistakes can be made during this process. Here are five common errors:
- Incorrect or Incomplete Patient Information: One common mistake is not filling out the patient's name, date of birth, social security number (if applicable), and contact information accurately. This can lead to issues with patient identification and insurance billing.
- Failure to Document the Incident Address or Location Correctly: Precise documentation of the incident location is crucial for legal and insurance purposes. Errors in this section can also impact the accuracy of public health statistics.
- Omission of Vital Signs or Medical History: Skipping the vital signs or medical history sections can hinder the medical personnel's ability to understand the patient's condition fully. This information is essential for making informed medical decisions.
- Incorrect Classification of the Incident: Proper categorization of the incident (e.g., non-emergent, emergent with lights and siren) is essential for record-keeping and analysis. Misclassification can affect response protocol evaluations and insurance claims.
- Signature Omissions: Forgetting to sign the report or to obtain the necessary signatures compromises the document's legal validity. This error can lead to disputes regarding the accuracy of the report or the care provided.
To avoid these mistakes, it's important to fill out the Ambulance Report form diligently and review it for completeness and accuracy before submission.
Documents used along the form
In the high-stakes, fast-paced environment of emergency medical services, the Ambulance Report form acts as a critical piece of documentation that can significantly impact patient care. It provides a detailed account of the patient's condition, treatment administered, and the circumstances surrounding the emergency incident. However, this pivotal document does not exist in isolation. Several other forms and reports often complement it, each serving a specific purpose in the continuum of patient care, legal documentation, and service evaluation. Here's a list of documents that frequently accompany an Ambulance Report:
- Patient Care Report (PCR): This comprehensive document provides a full narrative description of the medical care and observation given to the patient from the point of contact until transfer of care. It includes patient history, assessment findings, interventions, and the patient’s response to treatment.
- Medication Administration Record: A log that details all the medications given to the patient during transport, including dosages, routes, and times of administration. It's crucial for ensuring proper drug delivery and for cross-checking patient's medication history.
- ECG Strips: If the patient underwent cardiac monitoring, the ECG strips would be attached, providing a graphical representation of the electrical activity of the patient’s heart during transit.
- Refusal of Care Form: In instances where a patient refuses treatment or transport after an EMS team arrives on scene, this document is signed by the patient, acknowledging their refusal and the potential risks involved.
- Advance Directive/Living Will: If available, a copy of the patient's advance directive or living will, which outlines their wishes regarding treatment, might accompany the ambulance report, especially in critical or end-of-life situations.
- Interfacility Transfer Form: When a patient is transferred from one healthcare facility to another, this form provides receiving staff with information about the patient's condition, treatment provided en route, and reason for transfer.
- Incident Report: In the event of an unusual occurrence, such as a delay in response time, equipment failure, or an adverse patient outcome, an incident report would be filed alongside the ambulance report for internal review and quality improvement.
- Witness Statements: For cases involving trauma, accidents, or under law enforcement investigation, statements from witnesses collected at the scene may be attached to provide additional context and information about the incident.
These documents, while each serving a unique purpose, collectively contribute to a holistic view of the patient's emergency care experience. They ensure continuity of care, facilitate medical and legal audits, and support quality improvement initiatives. Understanding the role and importance of each document underscores the complexity and responsibility undertaken by emergency medical services in their mission to save lives.
Similar forms
Patient Care Record: Like the Ambulance Report form, the Patient Care Record documents detailed information about a patient's condition and treatment, focusing on their medical history, symptoms, vital signs, administered treatments, and transfer details. Both forms provide a comprehensive view of the patient's medical handling during an emergency or transfer scenario.
Emergency Medical Services (EMS) Run Sheet: This document parallels the Ambulance Report form in cataloging the chronological sequence of care provided by EMS personnel from the moment of dispatch to the arrival at the destination. It shares similar sections on patient information, services rendered, and observations made during care.
Medical Transfer Sheet: Very similar to an Ambulance Report, it outlines the specifics regarding patient transfers between facilities, including patient details, reason for transfer, and receiving facility information. It ensures continuity of care by detailing medical conditions and treatments just as the Ambulance Report does for emergency services.
Trauma Registry Form: While focused on trauma patients specifically, this form mirrors the Ambulance Report in its collection of patient demographics, incident specifics, clinical assessments, and outcomes. Both are vital for clinical documentation and further statistical analysis to improve healthcare services.
Prehospital Care Report: This report records the assessment and care provided to a patient before arriving at a healthcare facility, akin to the Ambulance Report. It includes narratives, vital signs, treatment administered on-site or en route, and patient outcomes, serving as a critical link in the patient care chain.
Medical Incident Report: Similar in purpose, this document is used to detail an incident involving a patient, recording injuries, symptoms, the treatment provided, and the responders involved. These reports assist in legal, administrative, and quality improvement processes, much like Ambulance Reports.
First Responder Report: This document records the initial assessment and care provided by the first responders on the scene. It shares similarities with the Ambulance Report by detailing the scene description, patient's condition, and the interventions performed before additional medical help arrives.
Emergency Department Transfer Form: When patients are moved from the emergency department to another facility or department, this form outlines patient information, reason for transfer, and medical history, similar to the Ambulance Report. It ensures seamless care transition by summarizing the emergency care provided and future care needs.
Dos and Don'ts
Filling out an Ambulance Report form is a critical process that ensures patients receive appropriate care and legal requirements are met. Here are essential do’s and don’ts to consider:
Do's:
- Be accurate and detailed: When documenting the patient's condition, the incident, and care provided, ensure every piece of information is accurate. Precision in details can significantly impact the patient's treatment and legal clarity.
- Use clear, legible handwriting: Although it might seem basic, legible handwriting ensures that everyone who reviews the report can understand the details. If the form is digital, ensure the information is entered correctly and review it for typos.
- Include all relevant information: Fill out every applicable section of the report. Don’t leave sections blank unless they genuinely do not apply to the situation. If unsure, it’s better to include extra information than to leave out something important.
- Respect patient confidentiality: Patient information is confidential and should be treated with the utmost respect. Only share the report with individuals who are authorized to view it, and ensure that it is stored securely.
Don'ts:
- Avoid making assumptions: Only document what you know and have observed. If you’re unsure about a detail, note it as such. Assumptions can lead to inaccuracies, which may have serious consequences.
- Don't omit details: Even if a detail seems minor, it could be medically or legally significant. If it concerns the patient's care, the incident, or observations on the scene, include it.
- Don't use abbreviations or jargon not widely accepted: Stick to commonly understood medical abbreviations and clear language. Ambiguities or misunderstandings from specialized jargon can affect patient care outcomes or legal interpretations.
- Don't delay filing the report: Timeliness is crucial, as the report could be needed urgently for patient care decisions or legal purposes. Complete and submit the ambulance report as soon as possible after providing patient care.
Misconceptions
When it comes to the Ambulance Report form, especially the type utilized by the Department of Health & Family Services in the State of Wisconsin, there are several misconceptions worth addressing. These misunderstandings can lead to confusion about the document's purpose, content, and the confidentiality of the information it contains.
- Ambulance forms are only useful for billing purposes. While it's true these forms play a crucial role in billing, their significance extends far beyond that. They provide a comprehensive record of the patient's condition, treatment administered by the EMS crew, and vital signs, serving as a crucial source of information for ongoing medical care.
- Only medical professionals can understand ambulance report forms. Although these forms contain medical terminology, they are structured to be understandable. Key information about the patient's condition, the care they received, and the incident leading to EMS services being called is presented in a way that can be deciphered with basic medical knowledge.
- All information on the ambulance report is publicly accessible. This is incorrect. Sections of the ambulance report form contain confidential patient information protected by statutes like Wis. Stat. 146.82(1). Access to these details is strictly controlled to safeguard patient privacy.
- Every ambulance report is the same. Each report is unique and tailored to the specific incident and patient involved. While the form used may be standardized, the details filled in reflect the individual circumstances and treatments related to each emergency.
- The form is only completed after the patient is transported. The process of filling out the form begins as soon as the EMS team engages with the patient, capturing details progressively through observation, treatment, and transport phases to ensure accuracy and completeness of the patient's medical record.
Understanding these points helps clarify the purpose and process of ambulance report forms, promoting better comprehension and respect for the confidentiality and complexity of emergency medical services documentation.
Key takeaways
Filling out an Ambulance Report form accurately is crucial in documenting patient care and ensuring seamless communication between emergency responders and health care facilities. Here are four key takeaways to consider:
- Completing the form is a requirement under administrative rule HFS 110.04(3)(b), emphasizing its importance in maintaining compliance with state regulations.
- The form contains sections that are confidential under Wis. Stat. 146.82(1), which highlights the need to handle patient information with care, respecting their privacy and confidentiality.
- It includes detailed sections on patient information, incident details, patient care record, crew member details, and more, requiring thorough and accurate input from emergency medical services (EMS) providers to ensure all relevant details are communicated effectively.
- The inclusion of specific data points like the Glasgow Coma Scale, Injury/Pain Location, and Incident Disposition underscores the comprehensive nature of the report, enabling caregivers to assess the patient's condition and response accurately.
In summary, the Ambulance Report form serves as a vital document in the EMS ecosystem, providing a structured way to record and transmit crucial patient care information. It aids in maintaining legal compliance, ensuring patient privacy, facilitating effective communication, and ultimately supporting the delivery of high-quality emergency medical care.
Popular PDF Forms
Dhs 3200 - Specifies the need for immediate contact with Centralized Intake if the report has not already been made by phone.
Da 31 Example - Functions as a valuable tool for military human resources in managing the dynamic allocation of duties.
Medicaid Expansion Nc - Key tool for adult care homes in North Carolina for facilitating Medicaid-covered patient admissions.