Blank Anesthesia Record PDF Template
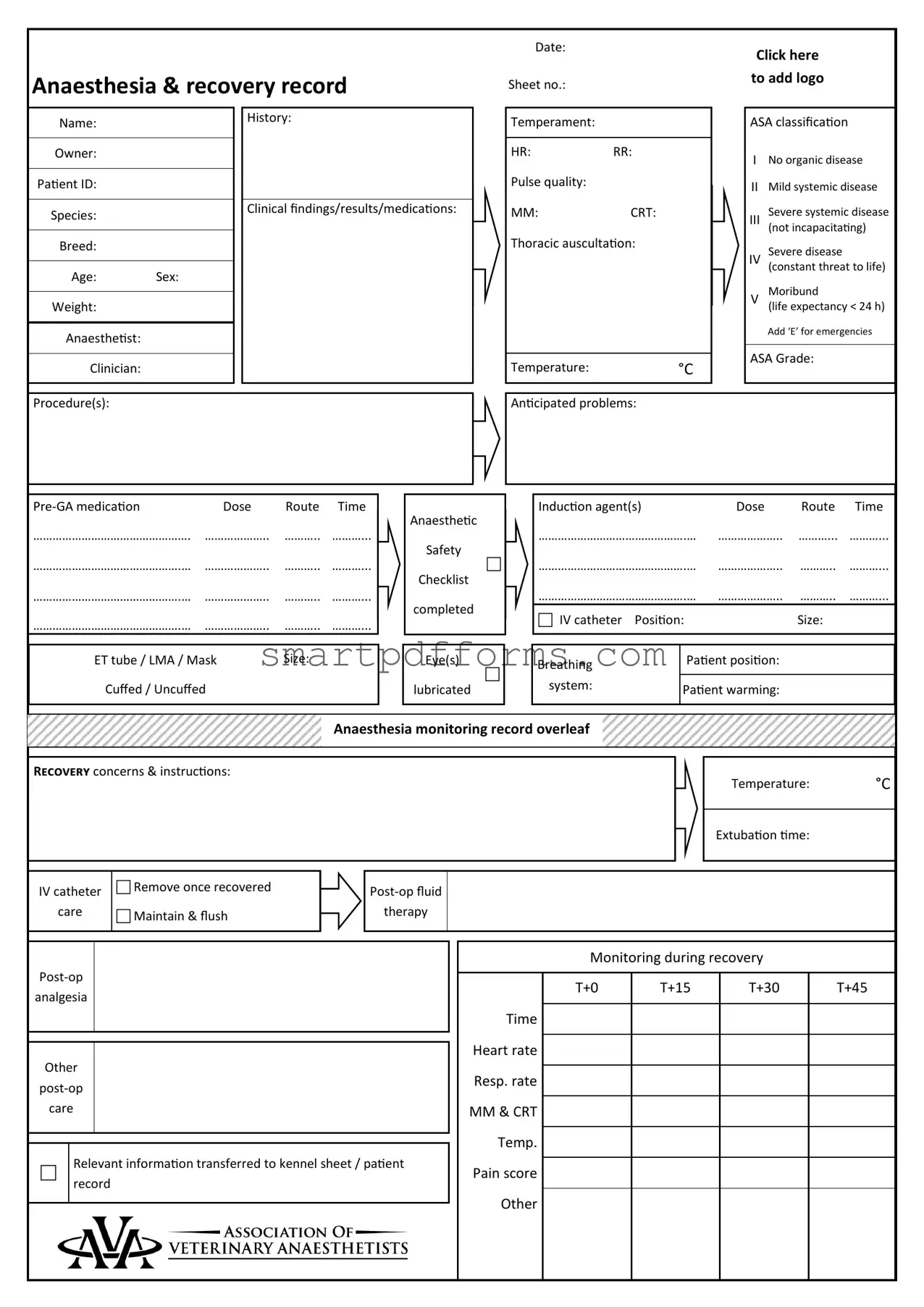
In the realm of veterinary medicine, the Anesthesia Record form plays a pivotal role, serving as a comprehensive document that charts every significant aspect of an animal's journey through anesthesia and recovery. This form includes a wide array of information, starting from basic identification details such as the patient's name, species, breed, age, and weight, extending to more nuanced data including the animal's medical history, temperament, and the American Society of Anesthesiologists (ASA) classification that assesses the anesthesia risk based on the patient's overall health status. It meticulously records pre-anesthesia evaluations like heart rate, respiratory rate, and findings from thoracic auscultation, alongside clinical findings and planned medications. The form also details the anesthesia process, noting the type and dosage of induction agents used, the equipment selected for airway management (endotracheal tube or laryngeal mask airway, for instance), and the patient's positioning during the procedure. Integral to ensuring patient safety is the inclusion of an anesthetic safety checklist and close monitoring of vital signs, which is documented throughout the procedure and into recovery, highlighting any concerns and instructions for post-operative care. This vigilance extends to monitoring the patient's temperature, heart and respiratory rates, mucous membrane color and capillary refill time, and pain score, thereby providing a critical tool for veterinarians to tailor post-operative care to each patient's needs. By encapsulating a detailed account of the entire anesthetic event from preparation through recovery, the Anesthesia Record form constitutes an indispensable tool in veterinary practice, ensuring the highest standards of patient care and safety.
Preview - Anesthesia Record Form
Anaesthesia & recovery record
Date:
Sheet no.:
Click here
to add logo
Name:
History:
Temperament:
ASA classification
Owner:
Patient ID:
HR:RR:
Pulse quality:
INo organic disease
IIMild systemic disease
Species:
Clinical findings/results/medications:
MM: |
CRT: |
Severe systemic disease
III
(not incapacitating)
Breed:
Age: Sex:
Weight:
Anaesthetist:
Clinician:
Thoracic auscultation: |
Temperature:°C
Severe disease
IV
(constant threat to life)
Moribund
V
(life expectancy < 24 h)
Add ‘E’ for emergencies
ASA Grade:
Procedure(s):
Anticipated problems:
|
|
|
Dose |
Route Time |
|
…………………………………………. |
……………….. |
……….. ………... |
……………………………………….… |
……………….. |
……….. ………... |
……………………………………….… |
……………….. |
……….. ………... |
……………………………………….… |
……………….. |
……….. ………... |
|
|
|
ET tube / LMA / Mask |
Size: |
|
Cuffed / Uncuffed |
|
|
|
|
|
Anaesthetic
Safety
Checklist
completed
Eye(s)
lubricated
|
|
|
|
|
|
|
Induction agent(s) |
|
Dose |
Route |
Time |
|
……………………………………….… |
……………….. |
………... |
………... |
|
|
……………………………………….… |
……………….. |
……….. |
………... |
|
|
……………………………………….… |
……………….. |
……….. |
………... |
|
|
IV catheter Position: |
|
Size: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Breathing |
Patient position: |
|
|
|
|
|
|
|
|
|
|
system: |
Patient warming: |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Anaesthesia monitoring record overleaf
Recovery concerns & instructions:
Temperature: °C
Extubation time:
IV catheter
care
Remove once recovered
Maintain & flush
therapy
analgesia
Other
care
Relevant information transferred to kennel sheet / patient record
Monitoring during recovery
|
T+0 |
T+15 |
T+30 |
T+45 |
Time |
|
|
|
|
|
|
|
|
|
Heart rate |
|
|
|
|
|
|
|
|
|
Resp. rate |
|
|
|
|
|
|
|
|
|
MM & CRT |
|
|
|
|
|
|
|
|
|
Temp. |
|
|
|
|
|
|
|
|
|
Pain score |
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|

|
|
Time |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Start procedure: |
Finish procedure: |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Throat pack |
Placed |
|
|
Removed |
||||||
|
|
Notes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
volume |
|
Total |
……………..………ml |
|
Dog |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10% |
……………..………ml |
85ml/kg |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Blood |
|
20% |
……………..………ml |
Cat / Rabbit |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
30% |
……………..………ml |
55ml/kg |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Notes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Key |
|
240 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
230 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HR |
● |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
220 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
o |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RR |
210 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
IPPV |
ø |
200 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
190 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
SAP |
˅ |
180 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
MAP |
– |
170 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
160 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
DAP |
˄ |
150 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
140 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Doppler |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
130 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
120 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Palpebral reflex |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
110 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Jaw tone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
100 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
90 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
80 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
70 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Eye position |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
60 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
↓ / → |
|
50 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
40 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
30 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Iso / Sevo |
|
% |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O2 / N2O / Air |
L/min |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Palpebral reflex |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Swabs |
|
|
|
|
|
Sharps |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Eye position |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
In |
|
Out |
|
|
|
In |
|
Out |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Jaw tone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pulse quality |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ETCO2 |
|
kPa/mmHg |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SpO2 |
|
% |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Temperature |
°C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Form Data
| Fact Name | Detail |
|---|---|
| Form Purpose | Anesthesia & recovery record |
| ASA Classification | Classifies patient health for anesthesia risk (I-V, add ‘E’ for emergencies) |
| Patient Identification | Includes name, species, breed, age, sex, weight, and patient ID |
| Medical Information | Covers history, temperament, clinical findings, medications, and anesthesia safety checklist completion |
| Anesthesia Monitoring | Tracks heart rate, respiratory rate, mucous membrane color, capillary refill time, temperature, pulse quality, and pain score |
| Anesthesia Administration | Details on pre-GA medication, induction agents, ET tube/LMA/Mask use, IV catheter details, patient positioning, and patient warming |
| Recovery Information | Includes recovery concerns, instructions, temperature, extubation time, IV catheter care, post-op fluid therapy, analgesia, and other post-op care |
| Procedure and Monitoring Graphics | Documents procedure start/finish times, total volume notes for blood loss estimation, monitoring graph key symbols, and anesthesia gas details |
Instructions on Utilizing Anesthesia Record
Filling out an Anesthesia Record form is essential for tracking the anesthesia process and patient response before, during, and after a medical procedure. This documentation aids in ensuring patient safety and enables healthcare providers to make informed decisions based on the patient's history and the specifics of their physical response to anesthesia. The Anesthesia Record form collects a wide range of data, from basic patient information to detailed anesthesia monitoring metrics. Here is a guide on how to fill it out effectively.
- Enter the Date and Sheet number at the top of the form to ensure that all records are accurately cataloged and easily retrievable.
- Click on the designated area to add a logo if required, which is typically the practice or hospital logo, to personalize and officially mark the document.
- Fill in the patient's Name, History of medical conditions, and Temperament, as these details provide context for the anesthesia plan.
- Classify the patient's physical status according to the ASA (American Society of Anesthesiologists) classification to assess anesthesia risks.
- Detail the Owner's information, Patient ID, and specifics like Species, Breed, Age, Sex, and Weight for identification and tailored anesthesia administration.
- List the Clinical findings, Results, and Mediations, including HR (Heart Rate), RR (Respiratory Rate), Pulse quality, MM (Mucous Membranes), and CRT (Capillary Refill Time) to outline the patient's pre-anesthesia condition.
- Fill in information about the procedure(s) being performed, anticipated problems, and any pre-GA (General Anesthesia) medication administered, including dosage, route, and time.
- Specify the Type of airway device used (ET tube, LMA, Mask), its Size, and whether it is Cuffed or Uncuffed.
- Confirm if the Anaesthetic Safety Checklist is completed and if the patient's eyes are lubricated to prevent dryness during anesthesia.
- Document details of the Induction agent(s) used, including dosage, route, and time, to initiate anesthesia.
- Indicate the IV catheter Position and Size, which is crucial for administering medications and fluids during the procedure.
- Describe the Patient's position, the Breathing system, and Patient warming measures to maintain body temperature.
- On the reverse side, record Recovery concerns & instructions and complete the Anaesthesia monitoring record, detailing the patient’s response during and post-procedure.
- Include any relevant Post-op care instructions, such as IV catheter care, fluid therapy, analgesia, and other support the patient might need.
- Ensure all Relevant information is transferred to the kennel sheet or patient record for continued care monitoring.
This comprehensive approach to filling out the Anesthesia Record form ensures that every aspect of the anesthesia process is documented. This documentation not only supports the immediate care team in providing patient-centered care but also serves as a critical record for future reference.
Obtain Answers on Anesthesia Record
- What is an Anesthesia Record form, and why is it used?
- What information is required on the Anesthesia Record form?
- How does the ASA classification on the form impact patient care?
- What are some anticipated problems that might be listed on the form, and why?
- How should the medication section of the form be filled out?
- What is the significance of recording patient monitoring data during anesthesia?
- What should be done if there are recovery concerns or special instructions?
An Anesthesia Record form is a detailed document used to track all the anesthesia-related aspects of a patient’s treatment before, during, and after a surgical procedure. It includes information on pre-anesthesia medication, induction agents, patient monitoring data, and post-operative care. This form ensures that all team members are informed of the patient's anesthesia history and current status, contributing to safer and more effective patient care.
The form requires comprehensive information, including the patient's name, identification, history, and clinical details such as heart rate, respiratory rate, and ASA classification. It also covers the details of the anesthesia procedure, including medications, doses, and routes, equipment used, and monitoring records. The form should be completed with detailed notes on the patient's recovery, including any concerns or instructions for post-operative care.
The ASA (American Society of Anesthesiologists) classification system helps assess the patient's pre-operative physical status, indicating the level of risk involved with anesthesia. Ranging from I (healthy) to V (moribund), with the addition of 'E' for emergency procedures, this classification guides the preparation and monitoring level required, ensuring tailored and appropriate care for each patient.
Anticipated problems might include potential reactions to anesthesia, complications based on the patient's medical history or physical examination, and concerns related to the specific procedure being performed. Listing these helps the medical team prepare for and quickly address any issues that arise, enhancing patient safety.
The medication section should include all pre-anesthesia medications, induction agents, and any other drugs administered related to anesthesia, with specific details on the dose, route, and time of administration. Accurately completing this section is crucial for tracking the patient's response to medications and managing any adverse reactions.
Recording patient monitoring data, such as heart rate, respiratory rate, blood pressure, and temperature, is vital for assessing the patient’s response to anesthesia and the procedure. This data helps in making real-time decisions about anesthesia depth, pain management, and fluid therapy, ensuring the patient's stability and safety throughout the surgical process.
If there are recovery concerns or special instructions, these should be clearly noted on the form for all team members involved in the patient's post-operative care. This includes details on extubation time, any complications observed, and specific instructions for IV catheter care, post-op fluid therapy, analgesia, or other necessary care. Clear communication and documentation are key to providing effective and safe post-operative recovery.
Common mistakes
Filling out an Anesthesia Record form is a critical part of preoperative preparation and postoperative care in medical settings involving anesthesia. However, mistakes can happen when completing this document. Here are some common errors:
Not updating the form with the date and sheet number can lead to confusion about when the anesthesia was administered and sequencing of multiple sheets.
Forgetting to add a logo or identifier for the clinic or hospital can make the form appear less professional and may lead to issues with form recognition and filing.
Omitting the patient's name, ID, or owner's information can result in a significant mix-up of records and potentially dangerous medical errors.
Failing to accurately record the ASA classification overlooks assessing the patient's preoperative risk, which is crucial for planning and executing anesthesia safely.
Skipping details about pre-GA medication, including dose, route, and time, compromises the ability to understand and evaluate the anesthesia plan and patient response.
Leaving the section on anticipated problems blank misses an opportunity to prepare for unexpected situations during the procedure.
Not noting the specifics about the patient's position, breathing system, or patient warming measures overlooks critical details that ensure the patient's safety and comfort.
Ignoring the recovery concerns & instructions can lead to inadequate postoperative care, affecting the patient's recovery and health outcome.
Avoiding these mistakes ensures that the anesthesia process is as safe and effective as possible. Here are some tips to remember:
Always double-check the form for completeness and accuracy.
Ensure that all medical staff involved in the procedure review and contribute to the record.
Use checklists to ensure no section of the form is overlooked.
By paying attention to these details, the risk of complications during and after anesthesia can be minimized, ensuring better patient care.
Documents used along the form
In the realm of healthcare, particularly within the fields of surgery and anesthesiology, various documents complement the Anesthesia Record to ensure a comprehensive and integrated approach to patient care. These documents facilitate communication among healthcare providers, enhance patient safety, and contribute to the smooth execution of surgical procedures. The Anesthesia Record itself captures detailed information about the anesthetic management of a patient throughout a surgical procedure, including pre-anesthetic medications, induction agents, patient monitoring data, and post-operative care instructions. Alongside this pivotal document, several others play key roles in patient care management.
- Pre-Anesthetic Evaluation Form: This document is used to assess a patient's medical history, physical examination findings, and laboratory test results prior to administering anesthesia. It helps in identifying any potential risks and planning the anesthetic strategy accordingly.
- Surgical Consent Form: Obtained from the patient or the patient's legal guardian, this form documents the patient's consent to undergo the specific surgical procedure, after being informed about the potential risks and benefits.
- Medication Administration Record (MAR): This comprehensive record tracks all medications administered to a patient, including the dosage, route, and time of administration, ensuring medication safety and adherence to the therapeutic plan.
- Pain Assessment and Management Chart: Essential for evaluating and managing the patient’s pain post-surgery, this chart records the patient's pain levels over time and the effectiveness of pain relief measures taken.
- Fluid Balance Chart: Monitoring a patient's fluid intake and output is crucial, especially in the perioperative setting. This chart helps in managing hydration status and detecting any imbalance that might require intervention.
- Post-Operative Care Plan: A document that outlines the tailored care instructions for a patient following surgery, including wound care, medications, activity level, and follow-up appointments.
- Surgical Operation Notes: This document provides a detailed account of the surgical procedure, including the surgical site, the steps of the operation, any complications encountered, and the outcomes. It’s crucial for post-operative care and for future reference.
- Discharge Summary: Upon a patient's discharge, this summary provides a concise overview of the hospital stay, including the reason for admission, course of treatment, condition at discharge, and follow-up care instructions.
- Patient Satisfaction Survey: Although not clinical in nature, this document enables patients to provide feedback on their care experience, which can be invaluable for healthcare providers in improving service quality and patient satisfaction.
The integration of these documents, including the Anesthesia Record, within the patient’s medical record, ensures a holistic view of the patient’s journey through surgery and recovery. Each document serves as a critical piece of the puzzle, contributing to a comprehensive approach that prioritizes patient safety, effective communication among healthcare providers, and the delivery of high-quality care. In the dynamic and complex environment of healthcare, meticulous documentation is indispensable for achieving the best possible patient outcomes.
Similar forms
Medical History Form: The Anesthesia Record form shares similarities with the Medical History Form in its collection of comprehensive patient history details. Both documents require information about the patient's past medical conditions, medications, and any underlying diseases, highlighted by the ASA classification on the Anesthesia Record. This classification reflects the patient's health status before anesthesia, akin to how a Medical History Form outlines potential health risks.
Operative Report: Like the Anesthesia Record, the Operative Report contains detailed information about the procedure performed, including the start and finish times, any complications encountered, and the outcome of the operation. The Anesthesia Record's inclusion of anticipated problems, the procedure(s) conducted, and notes on the procedure closely mirror elements of the Operative Report, providing a full picture of what occurred during surgery.
Medication Administration Record (MAR): The Anesthesia Record closely resembles the MAR due to its detailed logging of medications administered pre-, during, and post-operation, including the drug name, dose, route, and time. Both documents serve as critical tools for tracking patient medication schedules and ensuring proper dosages are given at the correct intervals, crucial for patient safety and effective treatment outcomes.
Pain Assessment and Management Chart: Both the Anesthesia Record and the Pain Assessment and Management Chart focus heavily on the patient's comfort and pain levels before, during, and after a procedure. The Anesthesia Record includes sections for monitoring pain scores, indicating a systematic approach to assessing and managing pain, much like the dedicated charts used in hospitals to ensure patients receive appropriate pain relief and care.
Dos and Don'ts
When filling out an Anesthesia Record form, it's important to ensure accuracy and completeness to provide the highest quality of patient care. Here are some dos and don'ts to consider:
Do:
- Review the form thoroughly before starting to ensure you understand all the sections and what information is required.
- Write legibly to ensure that anyone who reviews the form can easily understand the details of the anesthesia procedure and patient monitoring.
- Double-check all entries for accuracy, including patient information, anesthesia details, and any clinical findings or medication administered.
- Update the form in real-time or as close to real-time as possible to maintain an accurate record of the patient's condition and treatment.
Don't:
- Rush through the process . Taking your time to fill out each section accurately is crucial for the patient's safety and care quality.
- Skip sections that are applicable. If a section does not apply, mark it as such, but ensure that all relevant parts are completed in full.
- Use vague language in your descriptions. Be as specific and clear as possible to provide a precise account of the anesthesia process and patient's response.
- Forget to sign and date the form once completed. This verifies that the information is correct and has been reviewed by the responsible medical professional.
Misconceptions
Understanding the Anesthesia Record form is crucial for anyone involved in the medical care of animals, including pet owners. Here, we address seven common misconceptions about this important document.
Misconception 1: The form is only for veterinarians. While it's true that veterinary professionals primarily use the Anesthesia Record form, it's also a valuable tool for pet owners. It offers detailed insights into their pet's health status during anesthesia, which can be crucial for post-operative care.
Misconception 2: It's too complicated to understand. Although the form contains medical terminology, it's designed to be clear and straightforward. Key sections such as medications, dosages, and monitoring data are set out in a way that can be understood with some basic guidance.
Misconception 3: Only the anesthesia details matter. Every section of the form, from the patient's history to the recovery instructions, plays a vital role in ensuring the animal's safety and well-being. For instance, the ASA classification helps assess anesthesia risks, influencing care decisions.
Misconception 4: ASA classification is about the animal's age. The ASA classification reflects the animal's overall health and the risk associated with anesthesia, not just its age. This helps tailor the anesthesia plan to the individual animal's needs.
Misconception 5: The form doesn't include post-operative care. On the contrary, the form includes detailed sections on recovery concerns, instructions, and post-operative care, ensuring a smooth transition from anesthesia to recovery.
Misconception 6: If it's not written on the form, it's not important. While the form is comprehensive, it may not capture every nuance of the animal's condition or the procedure. Conversations with the veterinary team provide additional context and details not limited to the written record.
Misconception 7: It's a single-use document. The Anesthesia Record form is not just for the day of the procedure. It serves as a crucial part of the animal's medical history, informing future care and interventions.
Understanding the Anesthesia Record form is key to participating in your pet's care. It opens up a dialogue between pet owners and veterinary professionals, ensuring the best outcomes for the animal's health and well-being.
Key takeaways
Filling out the Anesthesia Record form accurately is critical for ensuring the safety and well-being of patients undergoing procedures that require anesthesia. Here are five key takeaways:
- Comprehensive Patient Information: The form begins with basic yet essential details, including the date, sheet number, and space for a logo. It is crucial to fill in the patient's name, ID, species, breed, age, sex, weight, and the owner's information accurately. This section helps in identifying the patient and ensuring that the anesthesia plan is tailored to their specific needs.
- Detailed Medical History and Physical Examination: A thorough history and physical examination, including temperament, ASA classification, clinical findings, medications, heart rate, respiratory rate, pulse quality, mucous membrane (MM) color, capillary refill time (CRT), thoracic auscultation, and body temperature, are vital. This information assesses the patient's overall health status and anesthesia risk, guiding the anesthesia plan.
- Anesthetic Plan Documentation: The form requires recording of pre-anesthesia medications, induction agents, and details regarding the endotracheal tube or mask used, including size and whether it is cuffed or uncuffed. Completing the anesthetic safety checklist and confirming eye lubrication are also important steps for patient safety. These details ensure that the anesthesia team is prepared and aware of all aspects of the plan.
- Anesthesia Monitoring and Recovery: On the back of the form, there's space to document ongoing monitoring during the anesthesia and recovery phase. This includes tracking time-based changes in heart rate, respiratory rate, MM & CRT, temperature, and pain score. Details on the patient's position, the breathing system used, patient warming methods, and any anticipated recovery concerns and instructions are also noted. Proper documentation here is crucial for patient monitoring and timely intervention if complications arise.
- Post-Operative Care Instructions: The form outlines post-operative care considerations, such as IV catheter care, post-op fluid therapy, analgesia, and other care instructions. Also, it emphasizes the importance of transferring relevant information to the kennel sheet or patient record. Ensuring that these instructions are well-documented and communicated to the entire veterinary care team supports a smooth recovery for the patient.
Accurately completing the Anesthesia Record form is a comprehensive process that demands attention to detail. It is an essential tool for safeguarding patient health during and after anesthesia, facilitating effective communication among the veterinary team, and providing a record for future reference.
Popular PDF Forms
Dot Long Form - Supports the CITY OF DALLAS's commitment to employing only the most qualified and reliable commercial drivers.
Renew Cosmetology License Ca - Ensure your cosmetology license renewal process in California is complete by not sending cash, only checks or money orders.
Connecticut 7B - Clarify your obligations under the Connecticut Workers’ Compensation Act using the 7B form when leading construction on your property.