Blank Asam Level Of Care Cheat Sheet PDF Template
The Asam Level Of Care Cheat Sheet form, also known as the Patient Placement Criteria Checklist - Kentucky Edition 2012, serves as a comprehensive tool for clinicians to appraise patient or client needs across six distinct dimensions before determining the appropriate level of care required for substance use disorder treatment. Adhering to the Adult Patient Placement Criteria-Second Edition Revised, this evaluation framework prioritizes addressing emergency needs first, aiming to place clients in the least intensive yet safe level of care that effectively facilitates their recovery goals. The form categorizes treatment services into several levels of care ranging from outpatient services, with less than six weekly service hours, to inpatient hospital settings, indicating the necessity for a more intense and clinically managed environment. Each level of care—identified as Level I through Level IV—outlines specific criteria regarding withdrawal potential, biomedical conditions and complications, severity of mental, emotional, behavioral, or cognitive conditions, readiness to change, risk for relapse or continued use, and the stability of the recovery environment. This structured approach ensures patients receive tailored treatment interventions, considering factors like Medication-Assisted Treatments (MAT), the individual's resistance or readiness for change, and the necessity for a supportive recovery environment. By meticulously assessing the needs based on these dimensions, the form guides clinicians in making informed decisions about the optimal level of care, whether it involves outpatient treatment, intensive outpatient services, transitional recovery centers, residential treatment, or inpatient hospital care.
Preview - Asam Level Of Care Cheat Sheet Form

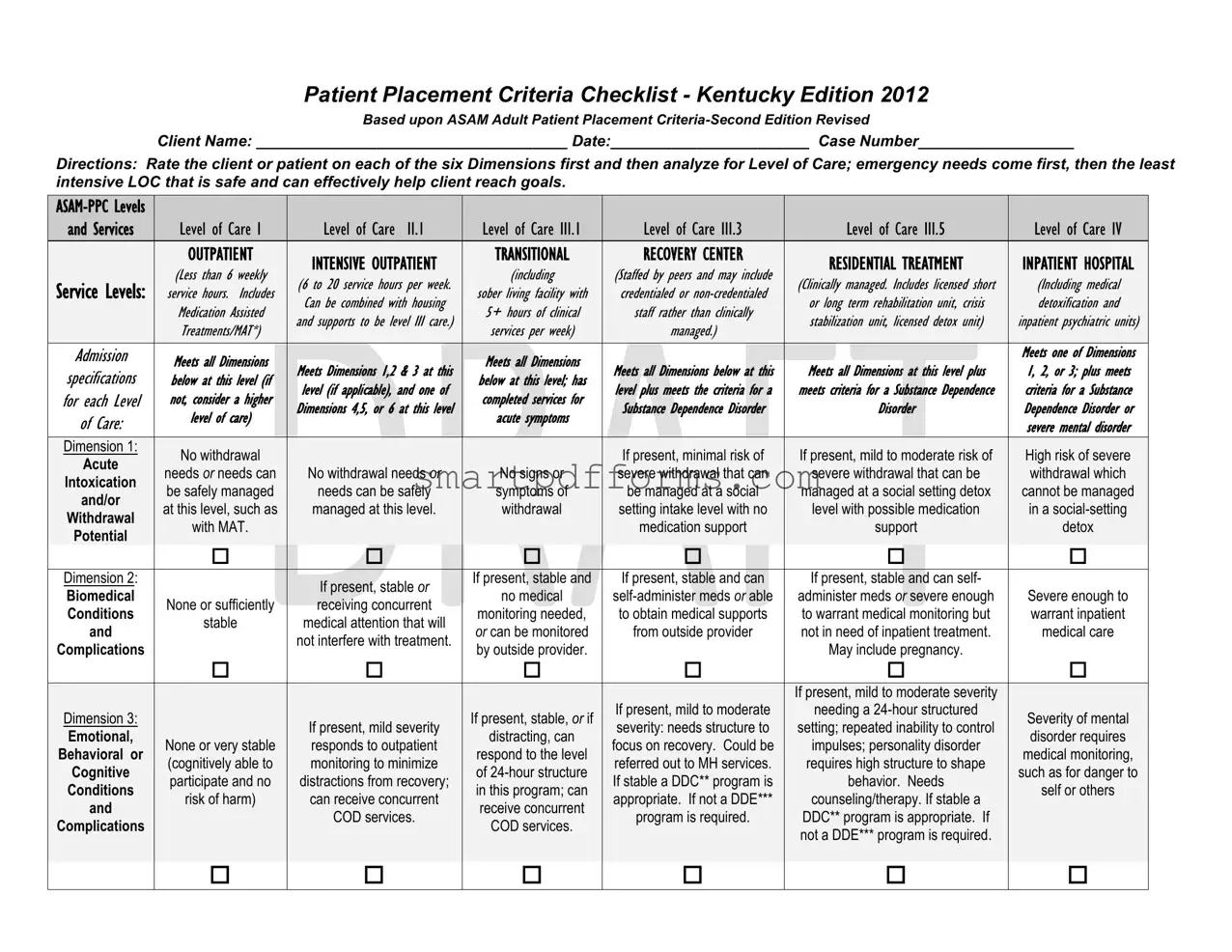
Patient Placement Criteria Checklist - Kentucky Edition 2012
Based upon ASAM Adult Patient Placement
Client Name: ____________________________________ Date:_______________________ Case Number__________________
Directions: Rate the client or patient on each of the six Dimensions first and then analyze for Level of Care; emergency needs come first, then the least intensive LOC that is safe and can effectively help client reach goals.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
and Services |
|
|
Level of Care I |
|
|
Level of Care |
II.1 |
|
|
Level of |
Care III.1 |
|
|
Level of |
Care III.3 |
|
|
Level of Care III.5 |
|
|
Level of |
Care IV |
|
|||||||
|
|
|
|
OUTPATIENT |
|
|
|
|
|
|
|
|
TRANSITIONAL |
|
|
RECOVERY CENTER |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
INTENSIVE OUTPATIENT |
|
|
|
|
RESIDENTIAL TREATMENT |
|
|
INPATIENT HOSPITAL |
|
||||||||||||||||
|
|
|
|
(Less |
than 6 |
weekly |
|
|
|
|
|
(including |
|
|
(Staffed by peers and may include |
|
|
|
|
|
|||||||||||
|
Service Levels: |
|
|
|
|
(6 to 20 service hours per week. |
|
|
|
|
|
|
|
(Clinically managed. Includes licensed short |
|
|
(Including medical |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
service |
hours. |
Includes |
|
|
|
|
sober |
living |
facility with |
|
|
credentialed or |
|
|
|
|
|
|||||||||||
|
|
|
|
|
Can be combined |
with |
housing |
|
|
|
|
or long term |
rehabilitation |
unit, crisis |
|
|
detoxification and |
|
|||||||||||||
|
|
|
|
Medication Assisted |
|
|
|
|
5+ |
hours |
of clinical |
|
|
staff rather |
than clinically |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
and supports to be |
level |
III care.) |
|
|
|
|
|
|
stabilization |
unit, licensed |
detox unit) |
|
|
inpatient psychiatric units) |
|
||||||||||
|
|
|
|
Treatments/MAT*) |
|
|
|
|
services per week) |
|
|
managed.) |
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Admission |
|
|
Meets |
all Dimensions |
|
|
|
|
|
|
|
Meets all |
Dimensions |
|
|
|
|
|
|
|
|
|
|
Meets one of Dimensions |
||||||
|
|
|
|
|
Meets Dimensions 1,2 & 3 at this |
|
|
Meets all Dimensions below at this |
|
Meets all Dimensions at this level plus |
|
1, 2, or 3; plus meets |
|||||||||||||||||||
|
specifications |
|
|
below |
at this |
level (if |
|
|
below |
at this level; has |
|
|
|
||||||||||||||||||
|
for each Level |
|
|
not, consider |
a higher |
|
level (if applicable), |
and one of |
|
completed |
services for |
|
level plus meets |
the criteria for a |
|
meets criteria for a Substance Dependence |
|
criteria for |
a Substance |
||||||||||||
|
|
|
|
Dimensions 4,5, or |
6 at this level |
|
|
Substance Dependence Disorder |
|
|
Disorder |
|
|
|
Dependence |
Disorder or |
|||||||||||||||
|
of Care: |
|
|
level of care) |
|
|
acute symptoms |
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
severe mental disorder |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Dimension 1: |
|
|
No withdrawal |
|
|
|
|
|
|
|
|
|
|
|
|
|
If present, minimal risk of |
|
|
If present, mild to moderate risk of |
|
|
High risk of severe |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Acute |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
needs OR needs can |
|
|
No withdrawal needs OR |
|
|
No signs or |
|
|
severe withdrawal that can |
|
|
severe withdrawal that can be |
|
|
withdrawal which |
|
||||||||||||
|
Intoxication |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
be safely managed |
|
|
needs can be safely |
|
|
symptoms of |
|
|
be managed at a social |
|
|
managed at a social setting detox |
|
|
cannot be managed |
|
||||||||||||
|
and/or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
at this level, such as |
|
|
managed at this level. |
|
|
withdrawal |
|
|
setting intake level with no |
|
|
level with possible medication |
|
|
in a |
|
||||||||||||
|
Withdrawal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
with MAT. |
|
|
|
|
|
|
|
|
|
|
|
|
|
medication support |
|
|
|
support |
|
|
|
detox |
|
|||||
|
Potential |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Dimension 2: |
|
|
|
|
|
|
|
If present, stable OR |
|
If present, stable and |
|
If present, stable and can |
|
If present, stable and can self- |
|
|
|
|
||||||||||||
|
Biomedical |
|
|
|
|
|
|
|
|
no medical |
|
|
administer meds OR severe enough |
|
Severe enough to |
||||||||||||||||
|
|
|
None or sufficiently |
|
receiving concurrent |
|
|
|
|
||||||||||||||||||||||
|
Conditions |
|
|
|
|
monitoring needed, |
|
to obtain medical supports |
|
to warrant medical monitoring but |
|
warrant inpatient |
|||||||||||||||||||
|
|
|
|
stable |
|
medical attention that will |
|
|
|
|
|||||||||||||||||||||
|
and |
|
|
|
|
|
OR can be monitored |
|
from outside provider |
|
not in need of inpatient treatment. |
|
medical care |
||||||||||||||||||
|
|
|
|
|
|
|
|
not interfere with treatment. |
|
|
|
|
|||||||||||||||||||
|
Complications |
|
|
|
|
|
|
|
|
by outside provider. |
|
|
|
|
|
May include pregnancy. |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If present, mild to moderate severity |
|
|
|
|
|
||
|
Dimension 3: |
|
|
|
|
|
|
|
|
|
|
|
|
|
If present, stable, OR if |
|
|
If present, mild to moderate |
|
|
needing a |
|
|
Severity of mental |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
If present, mild severity |
|
|
|
severity: needs structure to |
|
|
setting; repeated inability to control |
|
|
||||||||||||||
|
Emotional, |
|
|
|
|
|
|
|
|
|
distracting, can |
|
|
|
|
|
|
disorder requires |
|
||||||||||||
|
|
|
None or very stable |
|
|
responds to outpatient |
|
|
|
|
focus on recovery. Could be |
|
|
impulses; personality disorder |
|
|
|
||||||||||||||
|
Behavioral or |
|
|
|
|
|
|
respond to the level |
|
|
|
|
|
|
medical monitoring, |
|
|||||||||||||||
|
|
|
(cognitively able to |
|
|
monitoring to minimize |
|
|
|
|
referred out to MH services. |
|
|
requires high structure to shape |
|
|
|
||||||||||||||
|
Cognitive |
|
|
|
|
|
|
of |
|
|
|
|
|
|
such as for danger to |
|
|||||||||||||||
|
|
|
participate and no |
|
|
distractions from recovery; |
|
|
|
|
If stable a DDC** program is |
|
|
behavior. Needs |
|
|
|
||||||||||||||
|
Conditions |
|
|
|
|
|
|
in this program; can |
|
|
|
|
|
|
self or others |
|
|||||||||||||||
|
|
|
risk of harm) |
|
|
can receive concurrent |
|
|
|
|
appropriate. If not a DDE*** |
|
|
counseling/therapy. If stable a |
|
|
|
||||||||||||||
|
and |
|
|
|
|
|
|
receive concurrent |
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
COD services. |
|
|
|
|
program is required. |
|
|
DDC** program is appropriate. If |
|
|
|
|
|
||||||||||
|
Complications |
|
|
|
|
|
|
|
|
|
COD services. |
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
not a DDE*** program is required. |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||

CLIENT NAME:________________________________________________ DATE: _____________________ CASE NUMBER:________________________ ____
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Level of Care I |
|
|
Level of |
Care |
II.1 |
|
|
Level of |
Care III.1 |
|
|
Level of Care III.3 |
|
|
|
Level of Care III.5 |
|
Level of Care IV |
|
|||||||
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
OUTPATIENT |
|
|
INTENSIVE OUTPATIENT |
|
|
|
Transitional |
|
|
RECOVERY CENTER |
|
|
RESIDENTIAL TREATMENT |
|
INPATIENT HOSPITAL |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
(Less |
than 6 |
weekly |
|
|
(6 to |
20 service hours per |
|
|
|
(including |
|
|
(Staffed by peers and may include |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
(Clinically |
managed. Includes |
licensed short |
|
(Including medical |
|
||||||||||||
|
Service Levels: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
service |
hours. |
Includes |
|
|
week. Can |
be combined |
|
|
sober |
living |
facility with |
|
|
credentialed or |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
or long |
term |
rehabilitation |
unit, crisis |
|
detoxification and |
|
|||||||||||||
|
|
|
|
Medication Assisted |
|
|
with |
housing |
and |
supports |
|
|
5+ |
hours |
of |
clinical |
|
|
staff rather than clinically |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
stabilization |
unit, licensed |
detox unit) |
|
inpatient psychiatric units) |
|
|||||||||||||
|
|
|
|
Treatments/MAT*) |
|
|
to |
be level III |
care.) |
|
|
services per |
week) |
|
|
managed.) |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
Ready to change and |
|
Has marked difficulty with or |
|
|
Willing to cooperate |
Resistance is high |
Has little awareness & needs |
opposition to treatment, with |
||
|
cooperate at this |
|||||
|
or is ambivalent and |
enough to require |
interventions available only |
dangerous consequences; or there |
||
Dimension 4: |
level, OR externalizes |
|||||
needs motivation, |
structured program, |
at this level to engage & stay |
is high severity in this dimension but |
|||
Readiness to |
problems and needs |
|||||
recovery support, |
but not so high as to |
in recovery. May have |
not others. The client therefore |
|||
Change |
this level of structure, |
|||||
and monitoring |
render outpatient |
external leverage to support |
needs a motivational enhancement |
|||
|
motivation and |
|||||
|
strategies |
treatment ineffective. |
participation. |
program with 24 hour structure. |
||
|
support. |
|||||
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Has little awareness & needs |
|
|
|
|
|
|
|
|
|
|
|
Intensification of |
|
|
Client is at high risk |
|
intervention available only at |
|
Has little awareness & needs |
|
|
|
|
|
|
Able to maintain |
|
|
|
|
for imminent relapse |
|
this level to prevent |
|
intervention available only at this |
|
|
|
|
|
|
|
|
|
symptoms despite |
|
|
|
|
|
|
||||
|
Dimension 5: |
|
abstinence and |
|
|
|
|
with dangerous |
|
continued use, with |
|
level to prevent continued use, with |
|
|
||
|
|
|
|
active participation in |
|
|
|
|
|
|
||||||
|
Relapse, |
|
recovery goals or |
|
|
|
|
consequences. Client |
|
dangerous consequences to |
|
dangerous consequences to self or |
|
|
||
|
|
|
|
Outpatient, OR high |
|
|
|
|
|
|
||||||
|
Continued Use or |
|
achieve awareness |
|
|
|
|
needs |
|
self or others. |
|
others. |
|
|
||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
likelihood of relapse |
|
|
|
|
|
|
||||||
|
Continued |
|
of a substance use |
|
|
|
|
structure and support |
|
Does not recognize triggers, |
|
Does not recognize triggers, unable |
|
|
||
|
|
|
|
without close |
|
|
|
|
|
|
||||||
|
Problem Potential |
|
problem with minimal |
|
|
|
|
OR needs this support |
|
unable to control use, in |
|
to control use, in danger of relapse |
|
|
||
|
|
|
|
monitoring and |
|
|
|
|
|
|
||||||
|
|
|
|
support |
|
|
|
|
to transition into |
|
danger of relapse without |
|
without close |
|
|
|
|
|
|
|
|
|
support |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
community. |
|
close |
|
and structure. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
and structure. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Has a using, |
|
|
|
|
|
|
|
|
|
|
Supportive recovery |
|
|
Lacks social contacts |
|
|
unsupportive, |
|
Homelessness or lack of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
environment OR |
|
|
or social contacts |
|
|
dangerous, or |
|
|
Environment is dangerous or |
|
|
|
|
Dimension 6: |
|
|
|
|
|
|
|
safe, supportive recovery |
|
|
|
||||
|
|
|
willingness to obtain |
|
|
aren’t conducive to |
|
|
victimizing social |
|
|
unsupportive of recovery and client |
|
|
||
|
Recovery |
|
|
|
|
|
|
|
environment and client |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
such OR supports |
|
|
recovery, but with |
|
|
network, or lacks a |
|
|
lacks skills to cope outside of highly |
|
|
||
|
Environment |
|
|
|
|
|
|
|
needs |
|
|
|
||||
|
|
|
need professional |
|
|
structure or support, |
|
|
social network, |
|
|
structured |
|
|
||
|
|
|
|
|
|
|
|
|
learn to cope. |
|
|
|
||||
|
|
|
|
interventions. |
|
|
the patient can cope |
|
|
requiring this level of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Medication Assisted Treatments (MAT) can occur at any level of care and includes methadone, buprenorphine, and medications to control cravings and withdrawal when other criteria are met for level of care. Methadone and Suboxone clinics are generally outpatient, but clients on MAT may sometimes need a higher level of care.
**DDC: Dual Diagnosis Capable Program - has a primary target population of individuals with substance related disorders but also has an expectation and willingness to treat individuals with
referral to concurrent mental health services.
***DDE: Dual Diagnosis Enhanced Program – the program has the combined capacity to treat both mental health and substance related disorders equally.
Rater’s Signature: ____________________________________________________________
Last revision:
Form Data
| Fact Name | Description |
|---|---|
| Title and Purpose | The document is the "Patient Placement Criteria Checklist - Kentucky Edition 2012" and is based on the ASAM Adult Patient Placement Criteria-Second Edition Revised. It is designed to help rate a client or patient across six dimensions and then analyze the appropriate Level of Care (LOC). |
| Governing Law | This form is specifically tailored for use within the state of Kentucky, USA, following guidelines that align with the American Society of Addiction Medicine (ASAM) criteria adapted for state-specific requirements. |
| Levels of Care | The form outlines six distinct Levels of Care (I to IV), including outpatient services, intensive outpatient programs, various residential treatment options, and inpatient hospital care, catering to different intensities of addiction treatment needs. |
| Evaluation Criteria | Clients are evaluated across six dimensions, covering withdrawal potential, biomedical conditions and complications, emotional/behavioral/cognitive conditions, readiness to change, relapse potential, and recovery environment, to determine the most suitable level of care. |
Instructions on Utilizing Asam Level Of Care Cheat Sheet
Filling out the ASAM Level of Care Cheat Sheet form is an important step in determining the appropriate level of care for individuals with substance use disorders. Following the correct procedure ensures that the patient receives the best possible recommendation for their treatment plan. Here are the step-by-step instructions to accurately complete the form.
- Enter the client's information: Start by filling out the top section of the form with the client's name, date, and case number.
- Rate each of the six dimensions: The form requires you to evaluate the client on six different dimensions:
- Dimension 1: Withdrawal Potential
- Dimension 2: Biomedical Conditions and Complications
- Dimension 3: Emotional, Behavioral, or Cognitive Conditions and Complications
- Dimension 4: Readiness to Change
- Dimension 5: Relapse, Continued Use, or Continued Problem Potential
- Dimension 6: Recovery Environment
- Analyze for Level of Care (LOC): Based on the ratings given to each dimension, determine the appropriate Level of Care for the client. The form outlines six Levels of Care ranging from I (Outpatient) to IV (Inpatient Hospital).
- Mark the checkboxes next to the identified Level of Care for each dimension.
- Emergency needs consideration: Place a priority on emergency needs when they are present, before deciding on the least intensive Level of Care that is considered safe and effective for helping the client achieve their goals.
- Review Admission Criteria: Compare the client's ratings with the admission criteria specified for each Level of Care to ensure the chosen Level of Care is appropriate based on their needs.
- Sign the form: Once the assessment has been completed, sign the form at the bottom, verifying that the information provided and the determination made are accurate.
Keep in mind that this form is based on the ASAM Adult Patient Placement Criteria, allowing for a standardized approach to determining the most fitting treatment pathway for individuals battling substance use disorders. It is critical to approach each section of the form with careful consideration to ensure the client's needs are thoroughly addressed.
Obtain Answers on Asam Level Of Care Cheat Sheet
What is the ASAM Level of Care Cheat Sheet?
The ASAM Level of Care Cheat Sheet is a comprehensive tool designed to assist healthcare professionals in determining the most appropriate level of care for individuals dealing with substance use disorders. It's structured around the ASAM (American Society of Addiction Medicine) criteria, focusing on six key dimensions to assess patients' needs and place them into one of several levels of care, ranging from outpatient services to inpatient hospitalization.
How does the ASAM Cheat Sheet work?
The process starts by assessing the individual across six dimensions, including withdrawal potential, biomedical conditions, emotional/behavioral conditions, readiness to change, relapse potential, and recovery environment. Based on these assessments, healthcare professionals can identify the least intensive and most safe level of care (LOC) that effectively helps the patient move toward recovery. The form prioritizes emergency needs and aims for the patient to receive the appropriate level of support.
What are the six dimensions assessed by the ASAM Cheat Sheet?
The six dimensions include:
- Withdrawal potential
- Biomedical conditions and complications
- Emotional, behavioral, or cognitive conditions and complications
- Readiness to change
- Potential for relapse, continued use, or problematic use
- Recovery and living environment
Can you explain the different Levels of Care (LOC) in the ASAM Cheat Sheet?
Yes, the ASAM criteria outline several levels of care (LOC):
- Level of Care I: Outpatient services
- Level of Care II.1: Intensive outpatient services
- Level of Care III.1: Transitional Recovery Center
- Level of Care III.3: Residential treatment
- Level of Care III.5: Clinically managed high-intensity residential services
- Level of Care IV: Inpatient hospitalization
How do professionals decide which Level of Care is appropriate?
After conducting a thorough assessment across the six dimensions, professionals analyze the data to identify the safest and least restrictive setting where the individual can effectively work towards recovery goals. They also consider the intensity of services the patient requires and any emergency needs that might prioritize one level of care over another.
What does "Medication Assisted Treatments (MAT)" mean in the context of the ASAM Cheat Sheet?
MAT refers to the use of medications, in combination with counseling and behavioral therapies, to treat substance use disorders. This can include medications designed to control cravings and withdrawal symptoms. Within the ASAM framework, MAT can happen at any level of care, depending on other criteria met.
Can the ASAM Cheat Sheet be used for all patients?
While it's designed with adults in mind, the ASAM Cheat Sheet can be adapted to assess and place a wide range of patients dealing with substance use disorders. It's a flexible guide that aids in determining the best care approach based on individual needs and circumstances.
What does "emergency needs" mean in the context of the ASAM Cheat Sheet?
Emergency needs refer to immediate, critical situations that must be addressed before any other care decisions are made. This could involve managing severe withdrawal symptoms, dealing with acute medical or psychiatric conditions, or addressing any situation that might pose an immediate risk to the patient’s health or safety.
How often should the ASAM Level of Care assessment be completed?
Assessment frequency can vary based on the patient's progress, potential changes in their condition, or upon transition between levels of care. Continuous monitoring and periodic reassessment ensure that the patient remains in the most appropriate level of care to meet their evolving needs.
Who can perform an assessment using the ASAM Cheat Sheet?
Qualified healthcare professionals who are trained in the ASAM criteria, including but not limited to, addiction specialists, counselors, and psychiatrists, are equipped to perform assessments using the ASAM Cheat Sheet. These professionals ensure that assessments are comprehensive and accurately reflect the patient's needs.
Common mistakes
Filling out the ASAM Level of Care Cheat Sheet can be a complex process requiring attention to detail and an understanding of the patient's needs across several dimensions. Missteps in this process can lead not only to an inaccurate level of care recommendation but can also delay the patient's journey to recovery. Here are six common mistakes to avoid:
Overlooking client's emergency needs: Priority should always be given to immediate health or safety concerns. This includes serious withdrawal symptoms, suicidal ideation, or other acute conditions that might necessitate a more intensive level of care. Neglecting these urgent needs could result in harm to the client or others.
Misjudging the severity of withdrawal symptoms: Dimension 1 targets the client's potential withdrawal issues. Mistaking mild symptoms for severe ones, or vice versa, can lead to placing a client in an inappropriate level of care, either overwhelming them with unnecessary services or leaving them without the critical support they need.
Ignoring the client's biomedical conditions: Dimension 2 examines the client's physical health alongside their mental health issues. Failure to consider how biomedical conditions can affect mental health treatment, or vice versa, might compromise the effectiveness of the selected level of care.
Underestimating the impact of mental health issues: Dimension 3's focus on emotional, behavioral, and cognitive conditions requires a nuanced understanding of how these issues interact with substance use disorders. Placing a client without adequately considering these aspects can hinder their recovery by placing them in a treatment setting ill-suited to their mental health needs.
Miscalculating the client's readiness to change: Effectively assessing a client's motivation and readiness to engage in treatment is crucial for successful placement. An inaccurate assessment in Dimension 4 can result in a mismatch between the client's needs and the program's intensity, potentially leading to disengagement from the recovery process.
Overlooking the significance of the client's living environment: The client's recovery environment, addressed in Dimension 6, plays a vital role in their overall recovery process. Failing to recognize the need for a supportive and stable living situation can undermine recovery efforts, especially for clients who require a structured environment to maintain their sobriety.
By being mindful of these common errors and taking a holistic view of the client's needs across all six dimensions, practitioners can make informed decisions that enhance the effectiveness of treatment and support the client's path toward recovery.
Documents used along the form
When evaluating a person's needs concerning substance use and mental health treatment, a variety of forms and documents complement the ASAM Level Of Care Cheat Sheet form. These tools are integral in ensuring that individuals receive care that is not only suitable for their conditions but also respects their preferences and circumstances. Below is a brief overview of eight documents that are commonly used alongside the ASAM Level Of Care Cheat Sheet to facilitate a more comprehensive approach to patient care and evaluation.
- Consent to Treatment Form: This document is crucial as it records the patient's agreement to undergo the recommended treatment after being informed about the procedure, benefits, and potential risks.
- Privacy and Confidentiality Agreement: Essential for ensuring the patient understands their rights to privacy and how their personal and medical information can be used and shared.
- Patient Health Questionnaire (PHQ-9): A tool used to assess the presence and severity of depression, which can assist in the customization of the treatment plan.
- Substance Use Inventory: This detailed questionnaire evaluates the patient's history and patterns of substance use, offering insights necessary for selecting an appropriate level of care.
- Medical History Form: A comprehensive outline of the patient's medical background, including any ongoing treatments, allergies, and previous hospitalizations, to ensure safe and effective care planning.
- Treatment Agreement: This document outlines the responsibilities of both the patient and the treatment provider, setting clear expectations for the course of care.
- Crisis Intervention Plan: A proactive strategy designed to address potential emergencies, detailing steps to take in crisis situations to safeguard the patient.
- Discharge Summary and Plan: Prepared at the conclusion of a treatment phase, this summary reviews the care provided and outlines follow-up recommendations to support recovery.
Together, these supplementary documents ensure a holistic and respectful approach to treating individuals facing substance use and mental health challenges. They enable care providers to gather a broad spectrum of information, ranging from medical history to specific treatment preferences, thus fostering a safer and more effective care process that aligns with the individual's unique needs.
Similar forms
The Substance Abuse and Mental Health Services Administration (SAMHSA) Treatment Improvement Protocol (TIP) series documents are similar in that they also provide guidelines for determining appropriate levels of care for individuals with substance use and co-occurring disorders. Like the ASAM Level Of Care Cheat Sheet, these documents outline best practices for assessment, treatment planning, and service provision, emphasizing a continuum of care model.
The American Psychiatric Association (APA) Practice Guidelines for the Treatment of Psychiatric Disorders share similarities with the ASAM document as they offer comprehensive recommendations on the care and treatment of individuals with mental health disorders, including substance use disorders. Both sets of guidelines provide frameworks for clinical decision-making, and the APA guidelines extend this to psychiatric diagnoses specifically.
Behavioral Health Recovery Management (BHRM) project documents are similar in focusing on a recovery-oriented system of care for people with substance use and mental health conditions. They promote an integrated approach to treatment planning and service delivery, much like the ASAM Level Of Care Cheat Sheet, which advocates for a tailored approach to individual treatment needs.
The Joint Commission’s Behavioral Health Care Accreditation Standards are akin to the ASAM document in their focus on quality and safety in behavioral healthcare settings. Both documents emphasize evidence-based practices and patient-centered care, with the Joint Commission standards providing a framework for organizational structure and treatment environment quality.
The National Institute on Drug Abuse (NIDA) Principles of Drug Addiction Treatment presents principles of effective treatment of substance use disorders that resemble the ASAM criteria’s emphasis on evidence-based, individualized care. Both documents advocate for the integration of treatment services across different providers and care settings.
The Centers for Medicare & Medicaid Services (CMS) Regulations and Guidance documents, while broader in scope, relate to the ASAM document through their provisions on behavioral health services and support for individuals with substance use disorders. These federal regulations impact how services are delivered and reimbursed, influencing the implementation of ASAM criteria in clinical settings.
The Veterans Health Administration (VHA) Uniform Mental Health Services Handbook shares common goals with the ASAM Level Of Care Cheat Sheet in ensuring that veterans have access to a comprehensive array of mental health services, including substance use disorder treatment. Both documents guide the level of care determination and service provision based on individual need.
Lastly, The National Association of Addiction Treatment Providers (NAATP) Ethics Code complements the ASAM criteria by setting ethical standards for the treatment of individuals with substance use disorders, which the ASAM criteria implicitly support through its patient-centered, evidence-based approach to care decision-making.
Dos and Don'ts
When completing the ASAM Level of Care Cheat Sheet form, it’s crucial to ensure accurate and thoughtful completion to assist in appropriate patient placement. Below are guidelines on what you should and shouldn’t do when filling out the form.
Things You Should Do:
- Verify the patient's information (e.g., name, date, and case number) at the beginning to ensure it matches their records.
- Accurately rate the client or patient on each of the six dimensions before determining the Level of Care, basing your assessment on current and comprehensive data.
- Consider the least intensive Level of Care that is safe and likely to be effective, but prioritize addressing any emergency needs first.
- Utilize the descriptions provided for each Level of Care to guide your placement decision, ensuring it aligns with the patient’s needs.
- For patients with Substance Dependence Disorder or severe mental disorder, carefully analyze their conditions against the specified Level of Care criteria.
- Sign the form once completed to verify the accuracy of the assessment.
Things You Shouldn't Do:
- Rush through the assessment without thoroughly considering the patient's needs across all six dimensions.
- Overlook or underestimate the importance of accurately assessing Dimension 1 (Withdrawal) and Dimension 3 (Emotional, Behavioral, or Cognitive Conditions and Complications), as these are critical for correct Level of Care placement.
- Ignore the guidelines provided for outpatient, intensive outpatient, residential treatment, and inpatient hospital Levels of Care.
- Assume a higher Level of Care is better without considering the principle of placing a patient at the least intensive, but safe, Level of Care.
- Fill out the form based on incomplete or outdated information about the patient's condition.
- Forget to consider the external supports and environment (Dimension 6) which significantly impact the patient’s recovery process.
Misconceptions
Many people have misconceptions about the ASAM Level of Care Cheat Sheet form, especially when it pertains to its application and the information it provides. Highlighting these misunderstandings can clarify its purpose and usage.
- Misconception #1: The ASAM Cheat Sheet is Only for Medical Professionals.
While the form is designed with healthcare providers in mind, its structured approach to assessing patient needs helps ensure that individuals receive appropriate care based on standardized criteria. It is a resource for interdisciplinary teams, including social workers and recovery support specialists, to make informed decisions about patient care.
- Misconception #2: The Form Completely Automates Patient Placement Decisions.
Some may believe that the cheat sheet makes patient placement decisions automatic. However, the form is a guide to assist in making these decisions. The individualized nature of care requires professionals to use their judgment in conjunction with the criteria, taking into account the unique circumstances of each patient.
- Misconception #3: The Cheat Sheet Addresses Only Substance Abuse Issues.
Although substance abuse treatment is a significant focus, the form also considers the patient's mental health, physical health, and social needs. It is a holistic tool that recognizes the complex interplay of various factors affecting individuals seeking care for substance use disorders.
- Misconception #4: ASAM Levels of Care Are Rigid and Inflexible.
There is a misconception that once a patient is placed in a particular level of care, there is little flexibility for adjustment. The cheat sheet and ASAM's criteria encourage ongoing assessment and adjustment based on the patient's progress and changing needs, allowing for movement between levels of care as necessary.
- Misconception #5: The Cheat Sheet Covers All Aspects of Patient Placement.
While the cheat sheet is a comprehensive guide, it doesn't replace the need for detailed assessment and individualized treatment planning. It is a starting point that helps clinicians identify the most appropriate level of care but should be used alongside clinical judgment and other assessment tools.
Understanding these misconceptions allows for a better appreciation of the ASAM Level of Care Cheat Sheet form as a tool in facilitating the placement of patients in the most appropriate level of care for their recovery journey.
Key takeaways
The ASAM Level of Care Cheat Sheet form is a valuable tool designed to help professionals accurately determine the correct level of care needed for individuals dealing with substance-related disorders. Understanding how to properly use this form can significantly impact the treatment process, ensuring that clients receive the most appropriate care for their unique needs. Here are nine key takeaways about filling out and using this form:
- Individual assessment is critical: The form requires a thorough evaluation of the client across six dimensions before recommending a level of care. This ensures a comprehensive understanding of the client’s needs.
- Dimension-focused approach: Emphasizing six dimensions allows the evaluator to consider various aspects of the client's life, including withdrawal potential, medical conditions, mental health, readiness to change, relapse potential, and the recovery environment.
- Evaluating emergency needs first: Identifying and addressing any immediate risks or emergency needs is prioritized before determining the least intensive, safe, and effective level of care (LOC).
- Matching client needs with the correct level of care: The checklist assists in aligning the client’s specific needs with the most appropriate ASAM-PPC level, ranging from outpatient services to inpatient hospitalization.
- Flexibility in care levels: The form guides the user to consider different levels of care, acknowledging that a client’s needs might be best met in various settings, such as outpatient, intensive outpatient, residential treatment, or inpatient hospital.
- Medication-Assisted Treatment (MAT) considerations: MAT can be included at any level of care, highlighting the flexibility in addressing withdrawal and cravings, underscoring the form's adaptability to incorporate medical treatments into the care plan.
- Emphasis on Dual Diagnosis: The form distinguishes between Dual Diagnosis Capable (DDC) and Dual Diagnosis Enhanced (DDE) programs, emphasizing the need for specialized treatment considerations for clients with co-occurring mental and substance use disorders.
- Client readiness and environment factors: Acknowledging the importance of the client's readiness to change and the influence of their recovery environment, the form ensures these factors are considered when determining the appropriate level of care.
- Comprehensive yet focused assessment: While the form provides a structured approach to assessing client needs, it also allows for the professional judgment of the evaluator, emphasizing the importance of individualized care planning.
By carefully reviewing and filling out the ASAM Level of Care Cheat Sheet form, treatment providers can ensure a tailored and effective treatment path, suited to the individual’s specific situation, ultimately fostering a more successful recovery journey.
Popular PDF Forms
Hud1 - Plays a crucial role in the final stages of property buying, selling, and refinancing by providing a financial breakdown.
Florida State Tax - Geared towards facilitating quick and accurate tax return preparation to meet Florida's tax filing requirements.
Joint Custody in Florida Form - Petitioners can use the form to propose detailed custody and visitation arrangements to be considered by the court.