Blank Dc 628 PDF Template
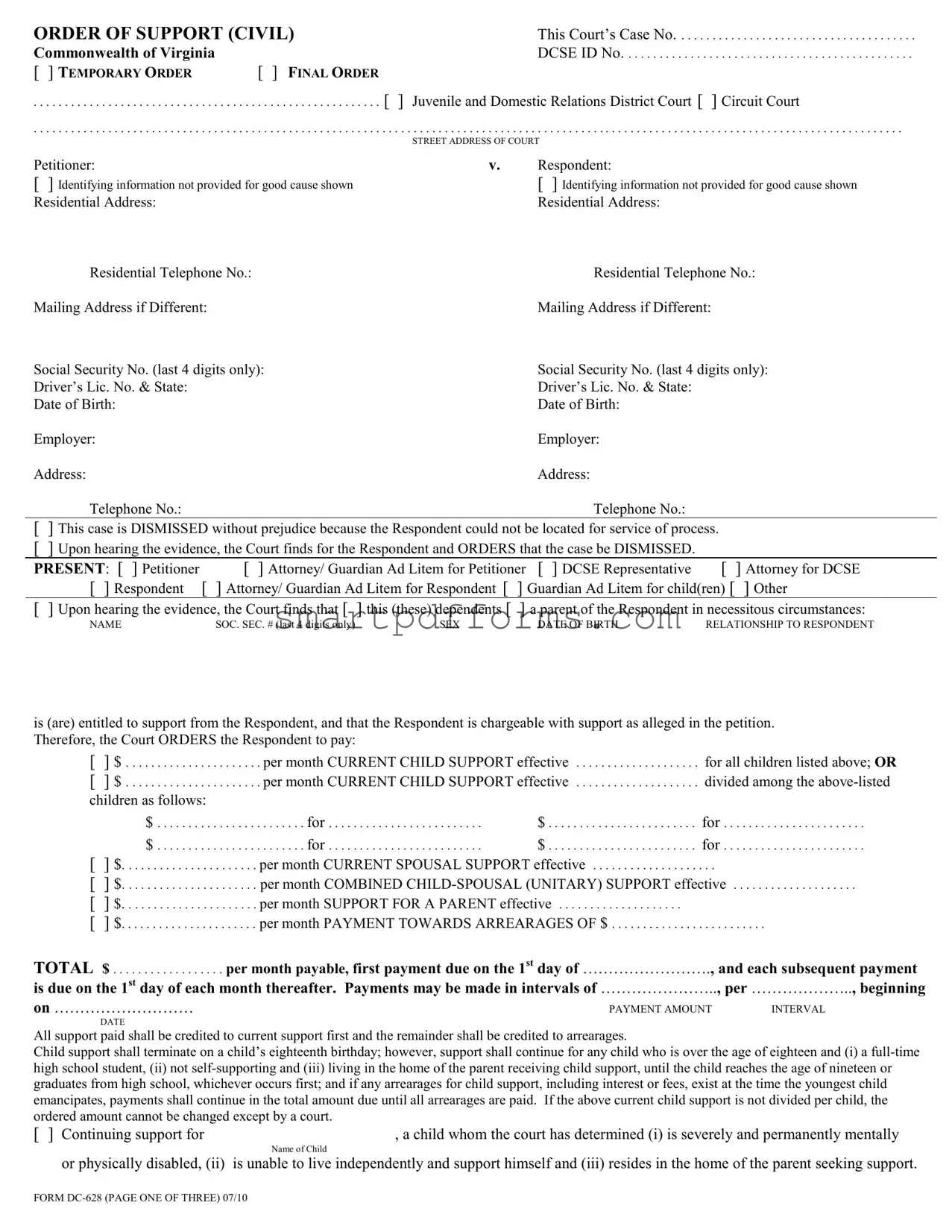
In the realm of legal and family support matters, the DC 628 Form, known as the "Order of Support (Civil)," plays a pivotal role within the Commonwealth of Virginia. Drafted and invoked by either the Juvenile and Domestic Relations District Court or the Circuit Court, this comprehensive document serves as the judicial articulation of obligations in support cases, which can include child, spousal, or parental support. It meticulously details each party's identifiers, such as addresses, contact numbers, and employment information, to ensure enforceability and compliance. What sets the DC 628 Form apart is its adaptability, offering provisions for both temporary and final orders, thereby accommodating the fluid dynamics of familial relationships and financial capacities. It encompasses arrangements for payment schedules, health care provisions, and even tax considerations, ensuring a holistic approach to support orders. Furthermore, it addresses potential future scenarios through stipulations for modifying support in response to significant changes in circumstances, reinforcing its forward-looking and comprehensive nature. Critical to both the payer and the recipient, this form outlines the legal responsibilities tied to support, the conditions under which these duties can be altered, and the repercussions for non-compliance, marking it as an essential document in the landscape of Virginia's family law.
Preview - Dc 628 Form

ORDER OF SUPPORT (CIVIL) |
This Court’s Case No |
|
Commonwealth of Virginia |
|
DCSE ID No |
[ ] TEMPORARY ORDER |
[ ] FINAL ORDER |
|
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . [ ] Juvenile and Domestic Relations District Court [ ] Circuit Court
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
STREET ADDRESS OF COURT
Petitioner: |
v. |
Respondent: |
[ ] Identifying information not provided for good cause shown |
|
[ ] Identifying information not provided for good cause shown |
Residential Address: |
|
Residential Address: |
Residential Telephone No.: |
|
Residential Telephone No.: |
Mailing Address if Different: |
|
Mailing Address if Different: |
Social Security No. (last 4 digits only): |
|
Social Security No. (last 4 digits only): |
Driver’s Lic. No. & State: |
|
Driver’s Lic. No. & State: |
Date of Birth: |
|
Date of Birth: |
Employer: |
|
Employer: |
Address: |
|
Address: |
Telephone No.: |
|
Telephone No.: |
[] This case is DISMISSED without prejudice because the Respondent could not be located for service of process.
[] Upon hearing the evidence, the Court finds for the Respondent and ORDERS that the case be DISMISSED.
PRESENT: [ ] Petitioner |
[ ] Attorney/ Guardian Ad Litem for Petitioner [ ] DCSE Representative |
[ |
] Attorney for DCSE |
[ ] Respondent |
[ ] Attorney/ Guardian Ad Litem for Respondent [ ] Guardian Ad Litem for child(ren) [ |
] Other |
|
[] Upon hearing the evidence, the Court finds that [ ] this (these) dependents [ ] a parent of the Respondent in necessitous circumstances:
NAME |
SOC. SEC. # (last 4 digits only) |
SEX |
DATE OF BIRTH |
RELATIONSHIP TO RESPONDENT |
is (are) entitled to support from the Respondent, and that the Respondent is chargeable with support as alleged in the petition. Therefore, the Court ORDERS the Respondent to pay:
[ |
] $ |
. . . . . . per month CURRENT CHILD SUPPORT effective |
for all children listed above; OR |
|
[ |
] $ |
. . . . . . per month CURRENT CHILD SUPPORT effective |
divided among the |
|
children as follows: |
|
|
|
|
|
$ |
. . . . . . . . . . . . . for |
$ |
for |
|
$ |
. . . . . . . . . . . . . for |
$ |
for |
[ |
] $ |
. . . . . per month CURRENT SPOUSAL SUPPORT effective |
. . . |
|
[ |
] $ |
. . . . . per month COMBINED |
||
[ |
] $ |
. . . . . per month SUPPORT FOR A PARENT effective |
|
|
[ |
] $ |
. . . . . per month PAYMENT TOWARDS ARREARAGES OF $ |
. . . . . . . . . . . |
|
TOTAL $ |
per month payable, first payment due on the 1st day of ……………………., and each subsequent payment |
|||
is due on the 1st day of each month thereafter. Payments may be made in intervals of ………………….., per ……………….., beginning
on ………………………
.PAYMENT AMOUNT |
INTERVAL |
DATE
All support paid shall be credited to current support first and the remainder shall be credited to arrearages.
Child support shall terminate on a child’s eighteenth birthday; however, support shall continue for any child who is over the age of eighteen and (i) a
[ ] Continuing support for |
, a child whom the court has determined (i) is severely and permanently mentally |
|
Name of Child |
or physically disabled, (ii) |
is unable to live independently and support himself and (iii) resides in the home of the parent seeking support. |
FORM

ORDER OF SUPPORT (CIVIL) |
Case No |
ARREARAGES:
[ ] No arrearages exist as of . . . . . . . . . . . . . . . . . .
[ ] $ . . . . . . . . . . . . . . . . . child support arrearage owed by Respondent. [ ] $ . . . . . . . . . . . . . . . . . spousal support arrearage owed by Respondent.
[ ] $ . . . . . . . . . . . . . . . . . unitary (child/spousal) support arrearage owed by Respondent.
[ ] $ |
total SUPPORT arrears owed by Respondent [ ] with interest included [ ] without interest included |
[] arrears include an assessment from the effective date of this order to the first payment due date.
[ ] This total includes TANF debt or other public funds paid prior to the effective date of this order of $ . . . . . . . . . . . . . . . . .
for . . . . . . . . . . . . months.
These arrearages are calculated as of the date of this Order including support owed for the current month. This amount does not include
payments made after ____/____/____, and respondent shall be credited for any payments made thereafter. Interest shall continue to accrue
on unpaid arrearages at the judgment rate unless the petitioner, in a writing submitted to the court, waives the collection of interest.
PAYMENT:
Payment shall be made payable to:
[] Petitioner at the address shown in the beginning of the Order.
The parties shall give the court at least 30 days written notice, in advance, of any proposed change of residential and, if different, mailing address and of any change of telephone number within 30 days of the change. The Respondent is required to keep the court informed of the name, address, and telephone number of his/her current employer.
[] Treasurer of Virginia and sent to Virginia Department of Social Services, Division of Child Support Enforcement, P.O. Box 570, Richmond, Virginia
1.Check or money order made payable to the Treasurer of Virginia.
2.Print on the check or money order:
Your name and social security number
Petitioner’s name as shown on the first page of this order
The DCSE ID No. shown on the first page of this order. If no such number is shown, use this Court’s name and case number as shown on the front page of this order until that number is sent to you; then start using the DCSE ID No.
The parties shall give to the Virginia Department of Social Services and the court, at least 30 days written notice, in advance, of any proposed change of residential and, if different, mailing address and of any change of telephone number within 30 days of the change. The Respondent is required to keep the Virginia Department of Social Services and the court informed of the name, address and telephone number of his/her current employer.
[] The parties shall also give each other at least 30 days written notice, in advance of any change of residential and, if different, mailing address and of any change in telephone number within 30 days after the change.
WARNING: Failure to pay in accordance with this order is a violation of this order and may be punished by a jail sentence or a fine or both. In addition, you may not receive credit for payments made contrary to the payment instructions provided in this order. Whenever income withholding is authorized, it is your responsibility to make the payment to DCSE until the income withholding becomes effective. You are responsible for keeping records of payments you make.
HEALTH CARE PROVISIONS:
[] Respondent [ ] Petitioner shall provide health care coverage for the [ ] child(ren) [ ] spouse and shall deliver the document necessary for the use of such coverage by the dependents
[] Respondent [ ] Petitioner shall provide dental care coverage for the [ ] child(ren) [ ] spouse and shall deliver the document necessary for the use of such coverage by the dependents
[] Respondent [ ] Petitioner presently has health care coverage and is ordered to maintain it or comparable coverage.
Health Insurance Company |
Policy name |
Name of Policy Holder |
Policy number |
In the event of any change in health insurance, the responsible party is required to notify the opposing party of the change. The responsible party shall inform the Virginia Department of Social Services, if support payments are ordered to be paid through the Virginia Department of Social Services, or the opposing party, if support payments are ordered to be paid directly to the opposing party, of any changes in the availability of the health care coverage for the minor child or children.
[] The Court finds that “health care coverage” as defined by the statute is not available at “reasonable cost” as defined by statute, and therefore, the Court does not order either the Respondent or the Petitioner to provide health care coverage.
[] Any reasonable and necessary unreimbursed medical and dental expenses for each child covered by this order shall be paid in the
following manner: . . . . . . . . . . . . . . % Respondent . . . . . . . . . . . . . % Petitioner.
FORM
ORDER OF SUPPORT (CIVIL) Case No. .............................................
[ ] Respondent [ ] Petitioner is ordered to execute the appropriate tax forms or waivers to grant the other party the right to take the
income tax dependency exemption for tax years . . . . . . . . . . . . . . . . . . . . . for . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CHILD OR CHILDREN
for federal and state income tax purposes.
[] The Court finds that a license, certificate, registration or other authorization to engage in a profession, business, trade, occupation, or
recreational activity issued by the Commonwealth of Virginia is held by
TYPE OF LICENSE |
AGENCY GRANTING LICENSE |
LICENSE NUMBER |
Respondent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Petitioner . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Upon a delinquency of a support payment for a period of 90 days or more, or in an amount of $5,000 or more, a petition may be filed for suspension of any license, certificate, registration or other authorization to engage in a profession, trade, business, occupation, or recreational activity issued by the Commonwealth. Virginia Code §
[ ] Withholding from income is ordered payable through the Virginia Department of Social Services by [ ] court income deduction order or [ ] administrative order for income withholding.
[] Immediate withholding from income is not ordered, pursuant to a written agreement between the parties or for good cause shown. It is further ORDERED that:
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
[ |
] This Order was determined based on [ |
] sole [ ] shared [ ] split custody guidelines. |
[ |
] A child support award of $ |
. . . . . . . . . . . . by application of the guidelines provided in Virginia Code § |
|
unjust or inappropriate in this case as determined by the relevant evidence pertaining to the factors set forth in the attached supplement |
|
|
which is incorporated herein by reference, the ability of each party to provide child support, and the best interest of the child. |
|
[] Entered in accordance with the parties’ written stipulation or agreement.
[ |
] The Respondent is also required to post with the Clerk a recognizance pursuant to § |
with/without surety |
|
[ |
] The Respondent shall also pay: $ |
reimbursement of costs to the Petitioner due . . |
. . . . . . . . . |
|
$ |
attorneys’ fees to the Petitioner’s attorney due |
. . . . . . . . . . . . . . . . . . |
If arrearage amount equals or exceeds 3 months owed, reasonable attorneys’ fees must be ordered pursuant to Virginia Code §
NOTICE: Support payments may be withheld as they become due from income without further amendment of this order or having to file an application for services with the Virginia Department of Social Services. Such order shall only be entered upon motion after proper notice sent by the clerk or counsel. Support payments may be withheld without further amendment of this order upon application for services with the Virginia Department of Social Services. In determining a support obligation, the support obligation as it becomes due and unpaid creates a judgment by operation of law. Failure to make payments when due means that interest will accrue according to Virginia Code § 6.1- 330.54.
The Virginia Department of Social Services may initiate a review of the amount of support ordered by any court. If a change in circumstances, as defined in the State Board of Social Services’ regulations, has occurred, the Department shall report its findings and a proposed modified order to the court which entered the order. Notice shall be served on both parties. Either party may request a hearing on the proposed modified order by filing a request with such court within 30 days of receipt of notice by the requesting party. Unless a hearing is requested with the time limits, no hearing shall be required and the modified order shall be effective 30 days after the notice is received and shall amend any prior court order. Virginia Code §
In cases enforced by the Virginia Department of Social Services, the Department of Motor Vehicles may suspend or refuse to renew the driver’s license of any person upon receipt of notice from the Virginia Department of Social Services that the person is delinquent in the payment of child support by 90 days or in an amount of $5,000 or more, or the person has failed to comply with a subpoena, summons, or warrant relating to paternity or child support proceedings.
If the order being reviewed by the Department deviates from the guidelines, based on one or more factors set out in Virginia Code §
THIS ORDER SHALL REMAIN IN FULL FORCE AND EFFECT UNTIL AMENDED OR ANNULLED BY THIS COURT OR A COURT OF COMPETENT JURISDICTION TO WHICH AN APPEAL MAY BE TAKEN.
. . . . . . . . . . . . . . . . . . . . . . . . . . . |
__________________________________________________________ |
DATE |
JUDGE |
SEEN AND AGREED AS TO NO PROVISION FOR INCOME WITHHOLDING.
PETITIONER:
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
RESPONDENT:
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
FORM
Form Data
| Fact Name | Detail |
|---|---|
| Type of Document | Order of Support (Civil) |
| Form Number and Revision Date | DC-628, revised July 2010 and July 2014 |
| Governing Law | Commonwealth of Virginia |
| Court Options | Juvenile and Domestic Relations District Court or Circuit Court |
| Types of Support Ordered | Temporary Order, Final Order, Current Child Support, Current Spousal Support, Combined Child-Spousal (Unitary) Support, Support for a Parent, Payment towards Arrearages |
| Specific Support Conditions | Provisions for child support continuation beyond the age of 18 under certain conditions, division of unreimbursed medical and dental expenses between parties, execution of tax forms for income tax dependency exemption |
| Payment Information | Details on payable party and address, instructions for check or money order details, warning about payment failure consequences |
| Unique Provisions | Criteria for support continuation for a child who is severely and permanently mentally or physically disabled, requirements for health care and dental coverage provision by one of the parties |
Instructions on Utilizing Dc 628
Filling out the DC-628 form, also known as the Order of Support (Civil), is a crucial step in legal proceedings regarding child, spousal, or parental support within the Commonwealth of Virginia. This document outlines the obligations of the respondent towards the petitioner in matters of financial support. It's important to provide accurate and complete information to ensure the order reflects the needs and circumstances of those it aims to protect.
- Start by entering the court's case number and the Commonwealth of Virginia DCSE ID No, if available. Specify whether this is a Temporary Order or a Final Order by marking the appropriate box.
- Indicate the type of court handling the case (Juvenile and Domestic Relations District Court or Circuit Court) by marking the corresponding box.
- Fill out the STREET ADDRESS OF COURT section with the court's complete street address.
- In the Petitioner vs. Respondent section, enter the full names of both parties involved. Note that identifying information can be omitted for good cause upon court approval.
- Provide the residential and, if applicable, mailing addresses for both petitioner and respondent. Include residential telephone numbers and the last four digits of both parties' Social Security Numbers, as well as their Driver's License Numbers and states of issuance. Include dates of birth and employer information for both parties.
- Mark the appropriate cause for case dismissal if applicable, or proceed to indicate attendance at the court hearing with a checkmark next to the relevant parties present.
- Under the support order section, list the dependents entitled to support. Include their names, last four digits of Social Security Numbers, sex, dates of birth, and relationships to the respondent. Specify the amounts for current child support, spousal support, combined support, or support towards arrearages as determined by the court.
- Enter the amount and interval of the payments, the due date of the first payment, and subsequent due dates for payments.
- On page two, specify any arrearages and how they are to be handled following the court's orders, including interest collection and TANF debt, if applicable.
- Choose the payment recipient—either the petitioner directly or the Treasurer of Virginia, through the Virginia Department of Social Services—and provide the address or P.O. Box accordingly. Also, include details required on the check or money order for payment.
- Address the healthcare provisions section by indicating which party is responsible for health and dental care coverage for children or spouse, and provide insurance company details if available.
- Complete the section about tax exemptions and licenses, identifying which party has the right to claim children as dependents for tax purposes and details on professional licenses held.
- Indicate if income withholding is ordered and provide details under the "It is further ORDERED that" section, including custody arrangements, guidelines deviations, and any requirements for recognizance.
- Fill out the final orders and agreements sections, including directives about maintaining records of payments, guidelines review by the Virginia Department of Social Services, and any special instructions provided by the court.
- Make sure the judge's signature, date, and any agreements between the petitioner and respondent regarding income withholding are included at the end of the form.
After filling out the form thoroughly, review all the information for accuracy. Submit the completed form to the appropriate court or legal authority as directed, ensuring you keep copies for your records and future reference.
Obtain Answers on Dc 628
What is a DC-628 form?
The DC-628 form, known as the Order of Support (Civil), is a legal document issued by a court in the Commonwealth of Virginia. It outlines the financial responsibilities, including child support, spousal support, and any arrearages, that a respondent must pay to a petitioner, as determined by the court. This form can establish temporary or final support orders and includes provisions for health care and tax considerations related to the dependents.
When is the DC-628 form used?
This form is used in cases where the court decides on matters of support, whether it be for a child, spouse, or both. It is applicable in both the Juvenile and Domestic Relations District Court and the Circuit Court. The form comes into play during legal proceedings concerning divorce, separation, or any scenario where a party is seeking financial support from another.
What kind of payments does the DC-628 form cover?
The DC-628 form covers various types of payments including:
- Current child support
- Spousal support
- Combined child and spousal (unitary) support
- Support for a parent
- Payments towards arrearages
How are child support payments determined and distributed according to the DC-628 form?
Child support payments are determined by the court based on guidelines laid out in the Virginia Code § 20-108.2. The court considers multiple factors, including the financial resources of both parents, the needs of the child, and custody arrangements. Payments are typically divided per child but can be ordered as a single sum for multiple children. The court also specifies how the payments are to be made, either directly to the custodial parent or through the Virginia Department of Social Services.
What happens if there are arrearages according to the DC-628 form?
Arrearages, or past due payments, are addressed on the form with the total amount owed by the respondent detailed. Interest on unpaid arrearages continues to accrue unless waived by the petitioner. The form also outlines the responsibility for covering any public funds paid, like TANF debt, before the effective date of the order.
How does the DC-628 form address health care coverage?
The form requires either the respondent or the petitioner to provide health and possibly dental care coverage for the dependents. It mandates the responsible party to maintain existing health coverage or obtain comparable new coverage. In scenarios where providing health care coverage is not deemed cost-effective by the court, no such order is made. Additionally, the form specifies how unreimbursed medical and dental expenses should be divided between the parties.
What are the legal consequences for non-compliance with a DC-628 order?
Failure to comply with the terms of a DC-628 order, including timely payment of support, may result in punitive actions such as fines, jail time, or both. Furthermore, the Virginia Department of Social Services can take measures including the suspension of driver's licenses or professional licenses for significant delinquency in support payments. Payments not made according to the order may not be credited, emphasizing the importance of adhering to the specified payment method and schedule.
Common mistakes
Filling out the DC 628 form, known as the Order of Support (Civil) for the Commonwealth of Virginia, is a critical step in the support case process. Avoiding common mistakes can streamline the process, ensuring timely and accurate support delivery. Here are ten mistakes to watch out for:
-
Not double-checking Court's Case No. and DCSE ID No.: These numbers are unique identifiers for your case. Mixing them up can lead to processing delays or misfiled documents.
-
Skipping the selection between Temporary and Final Order: Clearly indicating the nature of the order is crucial for its proper enforcement.
-
Omitting petitioner or respondent's identifying information: Although there are provisions for withholding this information for good cause, failing to provide it without proper reason can result in an incomplete filing.
-
Inaccurate financial information: Providing incorrect income or support payment amounts may lead to an unfair support order.
-
Neglecting to specify support allocation among dependents: If support is meant to be divided differently among children, this must be clearly detailed to avoid confusion.
-
Forgetting to include health care provision details: Health insurance is a significant factor in support calculations. Failing to document this properly can affect the dependents' well-being.
-
Misunderstanding the termination conditions for child support: Child support obligations have specific criteria for termination that must be thoroughly understood and correctly stated.
-
Incorrect payment details: Misidentifying the payee or method of payment can lead to missed or misdirected payments.
-
Failure to report changes in circumstances: All parties are obligated to inform the court of any significant changes that might affect support orders, such as employment status or residential changes.
-
Not complying with the order's administrative provisions: Failing to follow through on the procedural requirements like income withholding or executing tax forms can result in legal repercussions.
Addressing these common errors when completing the DC 628 form can help ensure that the support process proceeds smoothly for all involved parties.
Documents used along the form
When navigating the complexities of child and spousal support proceedings, various forms and documents are commonly required alongside the DC-628 form, each serving a specific purpose in the legal process. Understanding these documents can greatly assist individuals in preparing for their case, ensuring all necessary information is accurately presented to the court.
- DC-637: Child Support Guidelines Worksheet – This form helps calculate the amount of child support based on Virginia’s guidelines, considering both parents' income, childcare costs, and health insurance expenses.
- DC-4: Complaint for Support – Initiate a support case with this document, which outlines the petitioner’s request for child and/or spousal support.
- DC-454: Affidavit for Service of Process by Posting – Used when the respondent cannot be located, this affidavit allows for service by posting the notice at the courthouse.
- DC-635: Income Withholding Order (IWO) – Orders an employer to withhold a specified amount from the respondent's wages for support payments.
- DC-594: Motion to Amend or Review Order – Filed when either party seeks to have the support order reviewed for possible amendment due to changed circumstances.
- R-587: Financial Statement – A comprehensive form where a party discloses financial information, supporting the establishment or modification of support amounts.
- DCSE Application for Services – Application to the Division of Child Support Enforcement for assistance in obtaining, modifying, or enforcing a child support order.
- DC-168: Parenting Time Arrangement Form – Outlines the custody and visitation arrangement that can impact the child support calculation.
- DC-621: Notice of Registration of Foreign Support Order – Used to register a child or spousal support order from another jurisdiction for enforcement in Virginia.
- DC-572: Medical Support Notice to Employer – Informs an employer about the court-ordered requirement to enroll children in available health insurance plans.
Each of these documents plays a vital role in the proper adjudication and management of support cases. They ensure that all aspects of a party's financial responsibilities and rights are appropriately addressed. Individuals are encouraged to familiarize themselves with these forms and seek legal advice as needed to navigate their legal responsibilities and entitlements effectively.
Similar forms
Child Support Order Forms: Similar to the DC 628 form, child support order forms lay out the financial responsibilities a non-custodial parent has towards their child or children. These forms specify the amount of money to be paid for the child's care, how often payments should be made, and may include provisions for health insurance and educational expenses. Both documents are legally binding and enforceable through the court system.
Spousal Support (Alimony) Order Forms: These forms resemble the DC 628 in their function of specifying financial support, in this case, from one spouse to another following a separation or divorce. Such documents outline the amount of support, payment schedule, and duration of the support obligation. Spousal support orders, like the DC 628, can also address payment of arrearages and may include modifications based on changes in circumstances.
Income Withholding Orders: Income withholding orders are sent directly to an employer to garnish wages for child support, similar to some provisions of the DC 628 form. Both ensure timely payment of support obligations by automatically deducting the ordered amount from the obligor’s income. These documents serve a critical role in enforcing child support and spousal support orders by minimizing the delay or default on payments.
Arrearage Calculation Forms: These forms detail past due support payments, much like portions of the DC 628 that calculate arrearages owed by the respondent. They provide a breakdown of overdue payments, including principal and interest, if applicable. Both documents establish the total amount of arrearages to be paid and may include provisions for the payment method and schedule for clearing the outstanding balances.
Modification of Support Order Forms: These forms are used to request changes to an existing support order, analogous to sections of the DC 628 that might be used in case of modifications due to changed circumstances. They typically require evidence of a significant change in the financial situation of either party. Similar to the process outlined in the DC 628, these forms initiate judicial review and potentially adjust the support amounts in response to the new evidence presented.
Dos and Don'ts
Filling out legal forms can be a daunting process. Here are some essential dos and don'ts when dealing with the DC 628 form, the "Order of Support (Civil)" in Virginia, to help navigate the procedure more smoothly:
Dos:Read through the entire form first. Before you start filling it out, make sure you understand every section. This can help prevent mistakes and ensure you have all the necessary information at hand.
Use black ink. In most legal documents, black ink is preferred because it scans and copies clearly.
Provide accurate information. Whether it's personal details or financial information, ensure everything you enter is accurate and up-to-date.
Be thorough. Don't skip sections or leave blanks unless the form specifically instructs you to do so. If a section doesn't apply, consider entering "N/A" (not applicable) to indicate you didn't overlook it.
Include identifying numbers. Make sure to fill in the DCSE ID No and Court's Case No accurately, as these are critical for tracking and reference.
Check your math. If the form requires any calculations, double-check them for accuracy.
Sign and date the form. A legal document isn't usually valid without the appropriate signatures and dates.
Keep a copy for your records. Always keep a copy of the form and any attachments you submit.
Seek legal advice if unsure. If you're uncertain about any part of the form, consulting with a legal professional can help clarify your doubts.
Meet deadlines. If the form is part of a legal process with deadlines, make sure to submit it well before the due date to avoid any penalties.
Don't guess. If you're unsure about a section, it's better to seek clarification than to guess and risk providing incorrect information.
Don't use correction fluid or tape. Mistakes should be neatly crossed out and initialed, as correction fluid or tape can make it look like you're trying to hide information.
Don't provide false information. Falsifying information on a legal document can lead to serious legal consequences.
Don't overlook the payment instructions. Make sure you understand how and where payments should be made, as incorrect payments may not be credited properly.
Don't ignore the health care provisions. If you're responsible for providing health care coverage for dependents, ensure you comply with the specified requirements.
Don't leave parts incomplete. If a section is relevant to your situation, make sure you fill it out in full. Partially completed sections can cause delays.
Don't submit without reviewing. Always check over the form once you've completed it to ensure there are no mistakes or missing information.
Don't overlook the need for additional documentation. Some sections may require you to attach additional documents. Make sure these are complete and attached before submitting.
Don't forget to notify of address changes. If your residential or mailing address changes, make sure to notify the court and DCSE as required.
Don't ignore court orders or notices. If you receive further communication from the court or DCSE, don't ignore it. Respond promptly to avoid potential complications.
Misconceptions
Understanding legal documents is critical to navigating the judicial system effectively. Misconceptions about these documents can lead to confusion and missteps. The DC-628 form, an Order of Support in the Commonwealth of Virginia, is no exception. Below are ten common misconceptions about this form, clarified to foster a better understanding.
It's only about child support: While the DC-628 form is primarily used to order child support, it can also encompass spousal support, support for a parent, and combined child-spousal unitary support. The scope is broader than often perceived.
Orders are final and unchangeable: While the form does issue temporary or final orders, circumstances change, and so can the terms of the order. Modifications can be sought through the court if significant changes in circumstances occur.
It doesn't address health care provisions: The form includes provisions for health care and dental care coverage for children or spouses, demonstrating the court's comprehensive approach to dependent care beyond basic financial support.
Arrearages are simple to calculate: Arrearages, or past due support, include not just missed payments but also interest and, potentially, retroactive support amounts. This calculation can become complex, especially over long periods.
Payment methods are flexible: The order specifies payment methods and channels, such as directly to the Treasurer of Virginia or through the Division of Child Support Enforcement. Adhering to these instructions is crucial for ensuring proper credit of payments.
Paying directly to the custodial parent is always acceptable: Unless specified by the court, paying support directly to the custodial parent may not fulfill the legal obligation. Payments often need to be made through the designated state agency to be officially recognized.
Income withholding is a punitive measure: Withholding from income, or garnishment, is a standard enforcement tool, not a punishment. It ensures consistent support payments directly from the payer's income.
Child support only covers basic necessities: Child support is intended to cover a range of needs, including housing, food, clothing, educational costs, and healthcare. It's a contribution towards the overall costs of raising a child.
Child support automatically ends when a child turns 18: The form notes that support may continue beyond age 18 under certain conditions, such as the child being a full-time high school student, not self-supporting, and residing with the parent receiving support.
Failure to pay support is only a civil issue: While it's a civil order, failing to comply can lead to criminal penalties, including fines and imprisonment. Moreover, delinquency can trigger actions like license suspensions to enforce payment.
To navigate the complexities of legal obligations and rights, it's essential to understand documents like the DC-628 form clearly. Dispelling misconceptions helps parties involved make informed decisions and follow legal processes accurately.
Key takeaways
Filling out and using the DC 628 form, which is an Order of Support (Civil), plays a crucial role in the enforcement and modification of support orders within the Commonwealth of Virginia. Here are four key takeaways to understand about this document:
- The DC 628 form can be used to establish, modify, or enforce temporary or final support orders related to child support, spousal support, or a combined unitary support, ensuring the well-being of children and former spouses.
- Proper completion of this form requires accurate information about the petitioner and respondent's identification, including residential and mailing addresses, social security numbers (last four digits only), driver's license numbers, dates of birth, and employment details. This information facilitates effective communication and enforcement of the order.
- Payments, as ordered by the court, should be made to the Treasurer of Virginia and directed to the Virginia Department of Social Services, Division of Child Support Enforcement, unless otherwise stated. This ensures that support payments are processed and distributed efficiently and accurately.
- Failure to comply with the support order, including making timely payments as directed, can result in significant legal repercussions, including the possible suspension of licenses, certificates, or authorizations issued by the Commonwealth of Virginia. It further stresses the importance of adhering to the payment schedules and terms as dictated by the order.
Understanding and adhering to the requirements and instructions of the DC 628 form is essential for all parties involved in support order cases. It ensures that support is provided in a timely and efficient manner, upholding the best interests of those entitled to receive it.
Popular PDF Forms
Sc Dmv Form 452 - Essential for South Carolina vehicle owners needing to update or replace registration materials due to changes.
How Much Does It Cost to Join Amway - Clarifications on modifications to the terms of the IBO contract and the governing laws set the legal framework for the relationship between IBOs and Amway.
Bill Payment Processing Center Po Box 7236 Sioux Falls - Allows FIS BillPay customers to easily manage how they send funds to individuals, enhancing convenience and security.