Blank Dma 5199 PDF Template
In an effort to streamline the process of verifying eligibility for continued Medicaid or N.C. Health Choice coverage, the DMA-5199 form plays a pivotal role as a Medicaid Renewal Request for Information Notice. Dispatched by the County Department of Social Services (DSS), this form is a critical piece of documentation that seeks to gather comprehensive details about applicants and their immediate family members living in the household. It covers a broad spectrum of information, including tax filing status, dependency details, pregnancy, current Medicaid coverage, income, living conditions, and foster care history among others. Adequate completion of this form is imperative for applicants who wish to avoid the termination of their healthcare benefits, underscored by the requirement to respond within 30 days from the notice date. Additionally, the form provides avenues for adding more individuals in the household who require Medicaid coverage through Attachment A, thereby extending an opportunity to ensure that comprehensive health insurance coverage encompasses every eligible member within the household. Applicants are reminded of the serious nature of the information provided, as any submissions are under the penalty of perjury, stressing the importance of accuracy and truthfulness in the completion process. The flexibility in submission options—whether in person, by phone, or by mail—caters to the diverse needs and preferences of the applicant pool, ensuring that the process is as inclusive as possible.
Preview - Dma 5199 Form
Print Form
Medicaid Renewal Request for Information Notice
COUNTY DEPARTMENT OF SOCIAL SERVICES (DSS)
|
Date: _____________________ |
To: ______________________________________ |
|
Address: __________________________________ |
|
__________________________________ |
|
Case ID No: _______________________________ |
Worker: ____________________ |
*THIS FORM MUST BE SENT IN BY ____________________________ (30 DAYS FROM ABOVE DATE) OR YOU MAY LOSE YOUR N.C. MEDICAID OR N.C. HEALTH CHOICE *
Why You Need to Complete This Form
In order to be considered for Medicaid or N.C. Health Choice, you must complete this form. The information will be used to verify that you and your family still qualify. The information is necessary to process your review.
In addition to helping yourself, you can use this form to apply for health insurance coverage for other family members in your house.
Contact __________________ County DSS at ________________ if you have any questions about filling out
this form.
|
SECTION 1 |
|
|
TELL US ABOUT YOURSELF |
|
|
|
|
Do you expect to file a tax return? Yes |
No |
|
|
|
|
Are you a dependent on someone else’s tax return? Yes |
No |
|
|
|
|
If yes – who? |
|
|
|
|
|
SECTION 2
TELL US ABOUT YOUR FAMILY
(include family members and tax dependents living in your house)
PERSON 1:
Name:
Does this person expect to file a tax return? Yes  No
No
Does this person expect to be a dependent on someone else’s tax return? Yes  No
No 
If yes – who?
Is this person pregnant? Yes  No
No
If so, what is the expected due date?
Does this person have Medicaid? Yes  No
No 
1 |
If this person does not have Medicaid, complete Attachment A to apply for Medicaid.
PERSON 2:
Name:
Does this person expect to file a tax return? Yes  No
No 
Does this person expect to be a dependent on someone else’s tax return? Yes  No
No
If yes – who?
Is this person pregnant? Yes  No
No
If so, what is the expected due date?
Does this person have Medicaid? Yes  No
No 
To apply for Medicaid for this person complete Attachment A.
PERSON 3:
Name:
Does this person expect to file a tax return? Yes  No
No 
Does this person expect to be a dependent on someone else’s tax return? Yes  No
No 
If yes – who?
Is this person pregnant? Yes  No
No
If so, what is the expected due date?
Does this person have Medicaid? Yes  No
No
To apply for Medicaid for this person complete Attachment A.
PERSON 4:
Name
Does this person expect to file a tax return? Yes  No
No
Does this person expect to be a dependent on someone else’s tax return? Yes  No
No
If yes – who?
Is this person pregnant? Yes  No
No 
If so, what is the expected due date?
Does this person have Medicaid? Yes  No
No
To apply for Medicaid for this person complete Attachment A.
If more space is needed, please attach a separate sheet.
2 |
Medicaid Renewal Request for Information Notice
SECTION 3
TELL US MORE ABOUT THE PEOPLE LISTED ON THIS FORM
A.Income: Does anyone listed on this form have an income? Yes  No If yes, complete Attachment B.
No If yes, complete Attachment B.
B.Living Situation: Does anyone listed on this form live in a:
Long‐term care facility, group home, or nursing home
Private home, but gets at‐home medical, personal or health services
Private home, but gets medical, personal or health services in the community (such as adult day care)
If so, please list their names:
Name(s):
C.Foster Care: Is anyone listed on this form between the ages of 18 and 26 and was in foster care at
age 18? Yes  No
No 
If so, please list their names:
Name(s):
SECTION 4
SIGNATURE
I am signing this renewal form under penalty of perjury which means I have provided true answers to all the questions to the best of my knowledge. I know that I may be subject to penalties under federal law if I provide untrue information.
Beneficiary/Authorized Representative*
Date
*The person who completed the form or their legal representative.
|
WHERE TO SEND THE INFORMATION |
|
|
You can complete the form: |
|
|
|
• In‐person at the |
County DSS Office (street address) |
•By phone at:
• By mail at: |
County DSS Office, (mailing address) |
3 |
ATTACHMENT A
TO APPLY FOR MEDICAID FOR ANYONE LISTED IN SECTION 2.
Person 1:
A.Name:
B.Social Security Number:
C.Date of Birth:
D.How is this person related to you?
E.This person is : Male  Female
Female 
F.This person is a U.S. citizen or U.S. national Yes  No
No
If yes, skip to “additional information” below.
If no, answer question “G”:
G.If this person has eligible immigration status: Document Type:
ID Number:
 Check here, if this person has lived in the U.S. since 1996
Check here, if this person has lived in the U.S. since 1996
 Check here, if this person, his or her spouse, or a parent is a veteran or an active duty member in the U.S. military
Check here, if this person, his or her spouse, or a parent is a veteran or an active duty member in the U.S. military
Additional Information
 Check here, if this person lives with at least one child under the age of 19 and is the person taking care of this child.
Check here, if this person lives with at least one child under the age of 19 and is the person taking care of this child.
 Check here, if this person is 18 years or younger and has a parent living outside of the house
Check here, if this person is 18 years or younger and has a parent living outside of the house
 Check here, if this person wants help paying for medical bills from the last three months
Check here, if this person wants help paying for medical bills from the last three months
Person 2:
A.Name
B.Social Security Number
C.Date of Birth
D.How is this person related to you?
E.This person is : Male  Female
Female 
F.This person a U.S. citizen or U.S. national Yes  No If yes, skip to “additional information” below.
No If yes, skip to “additional information” below.
4 |
Medicaid Renewal Request for Information Notice
If no, answer question “G”
G.If this person has eligible immigration status: Document Type:
ID Number:
Check here, if this person has lived in the U.S. since 1996
 Check here, if this person, his or her spouse, or a parent is a veteran or an active duty member in the U.S. military
Check here, if this person, his or her spouse, or a parent is a veteran or an active duty member in the U.S. military
Additional Information
 Check here, if this person lives with at least one child under the age of 19 and is the person taking care of this child.
Check here, if this person lives with at least one child under the age of 19 and is the person taking care of this child.
 Check here, if this person is 18 years or younger and has a parent living outside of the house
Check here, if this person is 18 years or younger and has a parent living outside of the house
 Check here, if this person wants help paying for medical bills from the last three months
Check here, if this person wants help paying for medical bills from the last three months
If more space is needed, please attach a separate sheet.
5 |
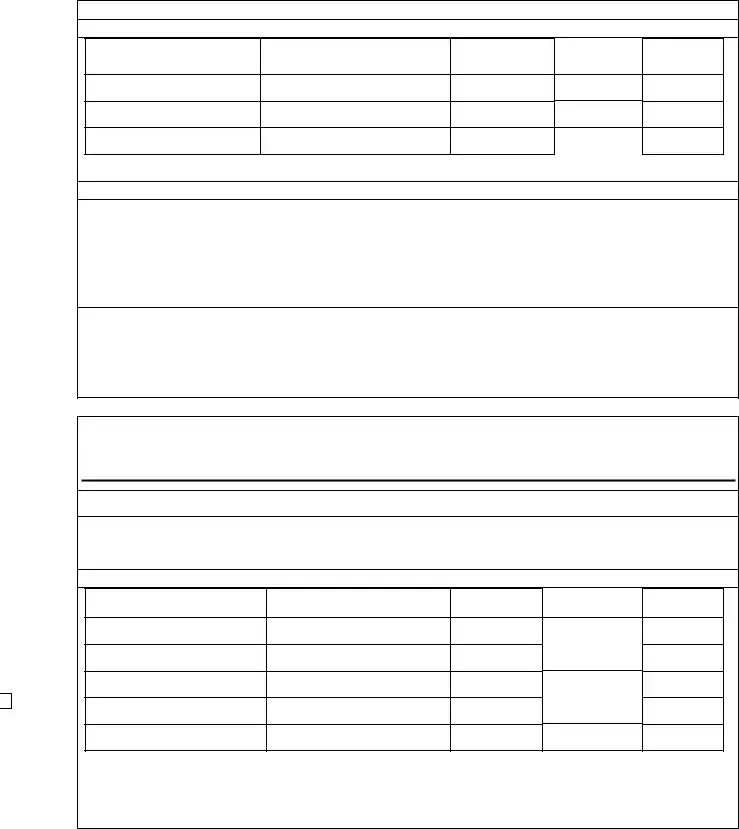
ATTACHMENT B
INCOME
Person Receiving Income
Income Type *
Amount
Before Taxes
How Often
Received
Start Date
If more space is needed to report changes, attach a separate sheet.
Include income from:
Jobs |
Foreign Income |
Self‐Employment |
Investment Income or Interest |
Alimony |
Farming or Fishing Income |
Unemployment |
Rental or Royal Income |
Social Security Benefits |
Capital Gains |
Retirement / Pension |
Scholarship |
Title |
Alien Sponsor |
Lump Sum Amount |
American Indian / Alaskan Native Income
Do not include:
Child Support
Workers Compensation
Supplemental Security Income (SSI)
Veterans Administration (VA) Benefits
C. Loss of Income: Was anyone listed on this form receiving income in the last 12 months but no longer is?
Yes  No
No 
If yes, who, when and what type?
D. Expenses: Is there anyone in the family deducting expenses from their taxes? Yes  No
No  If yes, complete Expenses (Deductions) below.
If yes, complete Expenses (Deductions) below.
EXPENSES (DEDUCTIONS)
Person Paying Deduction
Deduction Type
Amount
How Often
Start Date
If more space is needed to report changes, please attach a separate sheet.
6 |
Medicaid Renewal Request for Information Notice
Allowable deductions include: |
|
|
Alimony Paid |
Health Savings Acct Contributions |
Educator Expenses |
IRA Contributions |
Tuition / Fees |
Moving Expenses |
Student Loan Interest |
Penalty on Early Withdrawals of savings |
|
For those who are self‐employed, allowable deductions also include:
Rent / Royalty Expenses
Certain Business Expenses of Reservists, Performing Artists and Fee Basis Government Officials Deductible Part of Self‐Employment Tax
Domestic Production Activities Deduction Health Insurance Deduction
SEP, SIMPLE and Qualified Plans
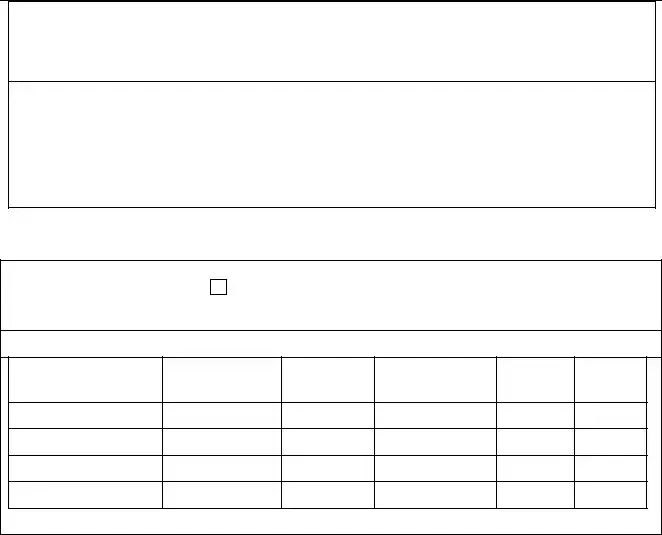
E. Health Insurance: Does anyone listed on this form have other health insurance besides Medicaid and
N.C. Health Choice? Yes  No
No
If so, complete Health Insurance below.
HEALTH INSURANCE
Person Covered
Policy Holder
Policy
Number
Insurance Company
Type of
Coverage
Start Date
If more space is needed to report changes, please attach a separate sheet.
Voter Registration:
If you are not registered to vote where you live now, would you like to apply to register to vote here today? __ yes __ no
If you want to register to vote, you can complete a voter registration form at http://www.ncsbe.gov/.
7 |
Form Data
| Fact Name | Description |
|---|---|
| Form Identification | DMA-5199, Medicaid Renewal Request for Information Notice |
| Issue Date | The form was last updated on March 30, 2016. |
| Purpose | To verify eligibility for continued Medicaid or N.C. Health Choice coverage by providing necessary information. |
| Submission Deadline | This form must be returned within 30 days from the date indicated at the top of the form to avoid potential loss of coverage. |
| Target Audience | Individuals or families currently enrolled in Medicaid or N.C. Health Choice seeking renewal of their coverage. |
| Key Sections | Contains sections for personal information, family details, income, living situation, and foster care status. |
| Attachments | Includes Attachment A for applying for Medicaid for persons listed in Section 2 and Attachment B for income verification. |
| Submission Methods | The form can be submitted in-person at a County DSS Office, by phone, or by mail as per the provided contact information. |
| Governing Law | North Carolina state laws govern the application and renewal process for Medicaid and N.C. Health Choice programs. |
Instructions on Utilizing Dma 5199
Filling out the DMA 5199 Medicaid Renewal Request for Information Notice is an important step in ensuring your continued eligibility for Medicaid or N.C. Health Choice coverage. Carefully completing this form is crucial for the assessment of your current situation and to determine if you and your family members still qualify for health benefits. Here's a straightforward guide to help you navigate through the form without missing any essential details.
- Start by noting the date at the top of the form where indicated.
- Fill in your full name, address, and Case ID No. in the spaces provided at the top of the form, under "To:".
- Mark the deadline given for submitting this form, as indicated by "*THIS FORM MUST BE SENT IN BY _________________".
- Section 1 - Tell Us About Yourself:
- Indicate whether you expect to file a tax return by checking "Yes" or "No".
- If you are a dependent on someone else’s tax return, check "Yes" and specify whose return it is. If "No", proceed to the next question.
- Section 2 - Tell Us About Your Family: For each family member, including yourself if applicable:
- Provide the name of the person.
- Answer whether this person expects to file a tax return and if they expect to be a dependent on someone else’s tax return, providing the name of the taxpayer if applicable.
- Indicate if the person is pregnant and provide the expected due date if applicable.
- Specify if the person currently has Medicaid. If not, you will need to complete Attachment A to apply for Medicaid for them.
- Section 3 - Tell Us More About The People Listed On This Form:
- Indicate whether anyone listed has an income by checking "Yes" or "No". If "Yes", complete Attachment B.
- Describe the living situation of anyone listed, specifying if they live in a care facility, receive at-home or community-based services, and list their names.
- If anyone listed was in foster care between ages 18 and 26, check "Yes" and list their names.
- Section 4 - Signature: Sign and date the form, affirming under penalty of perjury that the information provided is true. If someone other than the beneficiary completed the form, they should also sign as the authorized representative.
- Choose how you will send the information, noting the options provided (in-person, by phone, or by mail), and use the contact information for the County DSS Office provided on the form.
Once the form is completed and submitted by the deadline, your local County Department of Social Services will review the information provided to determine your continued eligibility for Medicaid or N.C. Health Choice. It's crucial to provide accurate and comprehensive information to avoid any delays or issues with your health coverage. If you have any questions or need assistance filling out the form, do not hesitate to contact your County DSS office as indicated on the form.
Obtain Answers on Dma 5199
What is the DMA-5199 form used for?
The DMA-5199 form is a Medicaid Renewal Request for Information Notice used by the county Department of Social Services (DSS) to verify if individuals and their families still qualify for Medicaid or N.C. Health Choice. Completing this form is necessary for the renewal process, and it can also be used to apply for health insurance coverage for other family members living in the same household.
When must the DMA-5199 form be submitted?
This form must be submitted within 30 days from the date noted on the form. Failing to submit the form within this timeframe may result in the loss of N.C. Medicaid or N.C. Health Choice coverage for you and potentially other family members.
What information is required on the DMA-5199 form?
The DMA-5199 form requires detailed information about you and your family members, including whether you or they expect to file a tax return, if any of you are dependents on someone else's tax return, and specific information about each family member such as pregnancy status and current Medicaid coverage. You'll also need to provide information on your income, living situation, and any children in foster care.
How can I submit the DMA-5199 form?
You have several options for submitting the DMA-5199 form. You can complete it in-person at the County DSS Office, by phone (contact information should be provided on the form), or by mail at the address listed for the County DSS Office on your form. Choose the method that is most convenient for you.
What happens if I provide false information on the DMA-5199 form?
Signing the DMA-5199 form under penalty of perjury signifies that all the information you've provided is true to the best of your knowledge. If you knowingly provide false information, you may be subject to penalties under federal law. It's crucial to ensure that all the information on the form is accurate and complete.
Common mistakes
Filling out the DMA 5199 form, which is crucial for Medicaid or N.C. Health Choice renewal, can sometimes be tricky. People often overlook or mishandle certain aspects, leading to errors that could potentially affect their eligibility or delay the process. Here are six common mistakes to avoid:
Missing the submission deadline: Not sending the form within 30 days from the date mentioned at the top can result in a loss of Medicaid or N.C. Health Choice coverage. It's vital to keep an eye on this timeframe to ensure continuous coverage.
Incomplete family information: Sometimes, sections relating to family members living in the house, including their tax status, pregnancy status, and whether they have Medicaid, are left incomplete or blank. This information is essential for a comprehensive review.
Incorrectly reported income: Failure to accurately report the income of everyone listed on the form, or neglecting to complete Attachment B when income is present, complicates the eligibility assessment.
Omitting details about living situations: The form queries about living arrangements to better understand your needs. Not specifying whether anyone lives in a long-term care facility, receives at-home services, or other specifics can lead to incomplete information.
Failure to mention foster care status: For individuals between the ages of 18 and 26 who were in foster care at age 18, forgetting to mention this status can cause them to miss out on potential benefits.
Signature omissions: The form must be signed, attesting to the accuracy of the information provided. Missing signatures, either from the beneficiary or the authorized representative, can invalidate the entire submission.
While filling out the DMA 5199 form, it's important to proceed carefully, ensuring that every piece of information is accurate and complete. Attention to detail can significantly smoothen the renewal process, securing healthcare benefits for you and your family.
Documents used along the form
When individuals or families apply for Medicaid or need to renew their Medicaid coverage, the DMA-5199 form is a key document. However, to ensure a thorough and accurate application process, several additional forms and documents are often required. These documents help verify eligibility, income, residency, and other crucial factors that influence Medicaid eligibility.
- Attachment A to Apply for Medicaid: This attachment is specifically for those listed in Section 2 of the DMA-5199 form who do not currently have Medicaid. It gathers detailed personal information including Social Security numbers, birth dates, and questions regarding U.S. citizenship or eligible immigration status.
- Attachment B - Income Verification: For anyone mentioned in the DMA-5199 form as having an income, Attachment B is necessary. This document collects information about sources of income, amounts, and frequency to assess financial eligibility for Medicaid.
- Proof of Residency: Applicants must prove that they are residents of the state in which they are applying for Medicaid. Acceptable documents might include utility bills, lease agreements, or state-issued identification cards.
- Birth Certificates: To verify ages and relationships within a household, birth certificates may be requested for all persons included in the Medicaid application.
- Proof of U.S. Citizenship or Immigration Status: Documentation is required to verify U.S. citizenship or lawful presence in the country. This may include U.S. passports, naturalization certificates, or green cards.
- Income Statements: Recent pay stubs, tax returns, or W-2 forms might be necessary to corroborate the income information provided in Attachment B.
- Proof of Disabilities or Health Conditions: If applicants are claiming eligibility based on disability or specific health conditions, medical records or letters from healthcare providers may be required.
- Foster Care Information: For individuals between 18 and 26 who were in foster care at age 18, documentation verifying this status is necessary for certain eligibility considerations.
- Proof of Pregnancy: If applicable, a medical statement or other document confirming pregnancy and the expected due date is needed.
Together, these documents support the DMA-5199 form in painting a complete picture of an applicant's circumstances. This comprehensive approach ensures that eligibility determinations are accurate and that all qualifying individuals and families receive the benefits they need. It's important for applicants to gather and submit this documentation promptly to avoid delays in their application or renewal process.
Similar forms
Medicaid Application Form: Much like the DMA-5199 form, the Medicaid Application Form is used to apply for Medicaid coverage. Both require personal, financial, and residency information to determine eligibility.
Health Insurance Marketplace Application: This form, used to apply for health insurance through the marketplace, mirrors the DMA-5199 in collecting details about family composition, income, and health insurance needs to identify appropriate coverage options.
Child Health Insurance Program (CHIP) Application: Similar to the DMA-5199, CHIP applications collect information on children’s health coverage needs, including tax filing status and dependent status, to provide low-cost health insurance to eligible children.
MAGI (Modified Adjusted Gross Income) Determination Form: This form, which assesses income for Medicaid and Health Choice eligibility, is similar to DMA-5199 in collecting financial information to verify eligibility for health coverage benefits.
Supplemental Nutrition Assistance Program (SNAP) Application: Though focusing on food assistance, SNAP applications resemble the DMA-5199 by requiring household, income, and residency information to establish eligibility for benefits.
Temporary Assistance for Needy Families (TANF) Application: Like the DMA-5199, TANF applications gather family composition, income, and other personal details to assist families in need with financial support.
Renewal/Redetermination Forms for Public Benefits: These forms, which are used for the ongoing verification of eligibility for benefits like Medicaid, share the goal of the DMA-5199 in periodically updating recipient information to ensure continued eligibility.
Medicare Savings Programs (MSP) Application: MSP applications, which help pay Medicare premiums, share similarities with the DMA-5199 in collecting financial and personal information to determine eligibility for Medicare cost assistance.
SSI/SSDI Application Forms: Applications for Social Security Disability Insurance (SSDI) and Supplemental Security Income (SSI) are similar to the DMA-5199 in that they require detailed personal and family information, including income, to establish eligibility for benefits.
Long-Term Care Medicaid Application: This specialized application shares the DMA-5199's requirement for comprehensive information on an individual’s health status, living arrangements, and financial status to determine eligibility for Medicaid coverage for long-term care services.
Dos and Don'ts
When it comes to filling out the DMA 5199 form for Medicaid or N.C. Health Choice renewal, it's important to approach the process with care and attention. Below are key dos and don’ts to guide you through the completion of this form efficiently and accurately.
- Do read through the entire form before starting to fill it out. This will give you a clear understanding of what information is required.
- Do gather all necessary documents and information beforehand, including income details, social security numbers, and any relevant tax information for you and your family members.
- Do answer every question as completely and accurately as possible. If a section does not apply to you, indicate with a "N/A" or "None" to show that you didn't overlook it.
- Do check if any additional attachments are needed (like Attachments A or B) for your application and include them with your form.
- Don't leave sections incomplete unless specifically instructed. Incomplete information could delay the processing of your form or affect your Medicaid eligibility.
- Don't guess on dates, amounts, or other factual information. If you're unsure, take the time to verify the correct information before submitting the form.
- Don't use correction fluid on the form. If you make a mistake, it's better to start over on a new form to ensure readability and prevent processing delays.
- Don't miss the submission deadline. Submitting your form by the due date is crucial to avoid losing your Medicaid or N.C. Health Choice coverage.
Remember, the accuracy and completeness of your DMA 5199 form are vital for maintaining your health coverage without interruption. Take your time, double-check your answers, and don't hesitate to reach out to your county's Department of Social Services (DSS) if you have any questions or need assistance.
Misconceptions
Understanding the DMA-5199 form is crucial for individuals seeking to renew their Medicaid or N.C. Health Choice coverage. However, there are several misconceptions surrounding this form that need to be addressed to ensure applicants can navigate the process more effectively.
Misconception #1: The DMA-5199 form is only for Medicaid renewals.
This form is not exclusively for Medicaid renewals; it also allows applicants to apply for N.C. Health Choice, catering to the needs of a broader audience than just existing Medicaid recipients.
Misconception #2: You don't need to provide information about your family members.
Contrary to this belief, the form requires detailed information about family members and tax dependents living in the household, highlighting its comprehensive approach to understanding an applicant’s situation.
Misconception #3: If you haven’t filed taxes, you cannot apply.
The form asks about tax filing status to understand an individual’s financial situation better but does not exclude non-filers from applying or renewing their Medicaid or N.C. Health Choice coverage.
Misconception #4: Submission deadlines are flexible.
A critical aspect of the form is its strict submission deadline—30 days from the date listed on the notice. Ignoring this deadline may result in the loss of coverage, emphasizing the importance of timely responses.
Misconception #5: Online submission is an option.
The DMA-5199 form outlines specific submission methods: in-person, by phone, or by mail. It does not provide an option for online submission, directing applicants towards more traditional methods.
Misconception #6: All sections must be filled out by everyone.
While the form is thorough, not all sections apply to every applicant. Sections are contingent on personal circumstances such as income levels, living situation, and whether any family member is in foster care, requiring a tailored approach to completion.
Misconception #7: You only need to sign the form if you are the beneficiary.
The form must be signed either by the beneficiary or an authorized representative, ensuring it is verified and authorized correctly, which is a crucial step in the submission process.
Misconception #8: Personal information isn’t verified.
One of the form's critical functions is to verify personal information provided by the applicant. Signing the form under penalty of perjury means that all information must be true and accurate, subject to verification.
Misconception #9: There is no need to list income sources.
Contrary to this belief, the form includes a section dedicated to income, which is essential for assessing eligibility and ensuring that support is allocated to those who truly need it.
Misconception #10: The form doesn’t accommodate non-citizens.
The DMA-5199 form has provisions for individuals with eligible immigration status, reflecting its inclusive approach. This acknowledges the diverse backgrounds of applicants, ensuring that non-citizens with eligible statuses can apply.
In summary, the DMA-5199 form is an essential document for individuals seeking to renew or apply for Medicaid or N.C. Health Choice. Dispelling these misconceptions is crucial for a smooth, successful application process, ensuring that all eligible individuals and families can access the coverage they need.
Key takeaways
Filling out the DMA 5199 form is a crucial step in the process of applying for Medicaid or N.C. Health Choice renewal. Here are six key takeaways to guide you through this process:
- Timeliness is key. You must send in this form by the specified deadline (30 days from the date noted at the top of the form) to avoid losing your N.C. Medicaid or N.C. Health Choice coverage.
- The information you provide on this form is essential for verifying your eligibility. This includes current information about you and your family members or tax dependents living in your house.
- It’s not just about you. Use the form to also apply for health insurance coverage for other family members in your household. This can include those not currently on Medicaid but who may be eligible.
- Income and living situation details matter. The form requires specific details about your income and living situation, impacting your eligibility and the specifics of your coverage. Make sure to complete Attachment B if anyone listed has an income.
- If applying for Medicaid for someone listed in Section 2, remember to complete Attachment A for each individual needing coverage. This includes providing details on their citizenship, U.S. national status, or eligible immigration status.
- The form must be signed under the penalty of perjury, emphasizing the importance of providing true and accurate information to the best of your knowledge.
You have multiple submission options: in-person at the County DSS Office, by phone, or by mail. Choose the method that is most convenient for you, but remember to keep track of the submission date to ensure it’s received before the deadline.
Popular PDF Forms
Commission Disbursement Authorization - Fosters a sense of security and trust among real estate professionals, knowing that financial agreements will be upheld.
Christian Cornerstone Correspondence School - Details regarding the student’s grade point average (GPA), class ranking, and graduation date can also be featured where applicable.