Blank Dmv Vision PDF Template
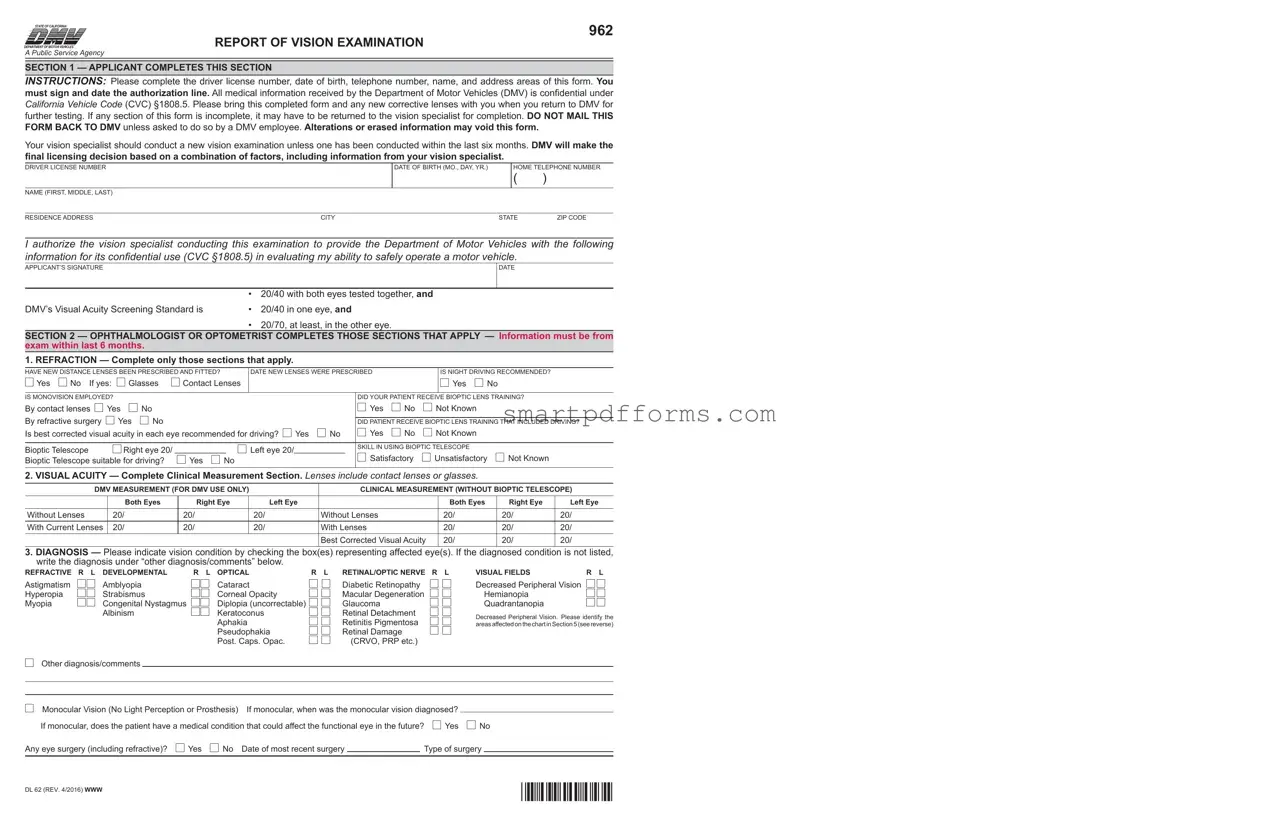
The Department of Motor Vehicles (DMV) in California provides a critical public service by ensuring that all drivers on the road have met specific safety standards, including visual acuity. The DMV Vision Form, known formally as the 962 Report of Vision Examination, plays a pivotal role in this process. It is a comprehensive document that applicants must complete with the assistance of a licensed vision specialist. This form requires detailed information from both the applicant and the vision specialist, including the driver's personal identification details, the results of their vision examination, and any prescriptive corrective measures necessary for driving. The form further delves into specifics such as the applicant’s ability to drive at night, the use of bioptic telescopes, and the overall analysis of their visual acuity with or without lenses. Moreover, the medical professional must report on any diagnosed vision conditions and their prognostic outlook, helping the DMV to understand the potential future impacts on the driver's visual capabilities. Importantly, all medical information shared through this form is treated as confidential, adhering to the protections outlined under California Vehicle Code (CVC) §1808.5. Ultimately, the DMV uses the information from this form, alongside other factors, to make an informed decision regarding an individual's ability to safely operate a motor vehicle. The meticulous structure of the DMV Vision Form thus underscores its importance in prioritizing road safety and the well-being of the driving community.
Preview - Dmv Vision Form
STATE OF CALIFORNIA
DEPARTMENT OF MOTOR VEHICLES®
A Public Service Agency
962
REPORT OF VISION EXAMINATION
SECTION 1 — APPLICANT COMPLETES THIS SECTION
INSTRUCTIONS: Please complete the driver license number, date of birth, telephone number, name, and address areas of this form. You must sign and date the authorization line. All medical information received by the Department of Motor Vehicles (DMV) is conidential under
California Vehicle Code (CVC) §1808.5. Please bring this completed form and any new corrective lenses with you when you return to DMV for further testing. If any section of this form is incomplete, it may have to be returned to the vision specialist for completion. DO NOT MAIL THIS FORM BACK TO DMV unless asked to do so by a DMV employee. Alterations or erased information may void this form.
Your vision specialist should conduct a new vision examination unless one has been conducted within the last six months. DMV will make the inal licensing decision based on a combination of factors, including information from your vision specialist.
DRIVER LICENSE NUMBER
NAME (FIRST, MIDDLE, LAST)
DATE OF BIRTH (MO., DAY, YR.)
HOME TELEPHONE NUMBER
()
RESIDENCE ADDRESS |
CITY |
STATE |
ZIP CODE |
I authorize the vision specialist conducting this examination to provide the Department of Motor Vehicles with the following
information for its conidential use (CVC §1808.5) in evaluating my ability to safely operate a motor vehicle.
APPLICANT’S SIGNATURE
DATE
|
• |
20/40 with both eyes tested together, and |
DMV’s Visual Acuity Screening Standard is |
• |
20/40 in one eye, and |
• 20/70, at least, in the other eye.
SECTION 2 — OPHTHALMOLOGIST OR OPTOMETRIST COMPLETES THOSE SECTIONS THAT APPLY — Information must be from exam within last 6 months.
1. REFRACTION — Complete only those sections that apply.
HAVE NEW DISTANCE LENSES BEEN PRESCRIBED AND FITTED?
Yes |
No If yes: |
Glasses |
Contact Lenses |
DATE NEW LENSES WERE PRESCRIBED
IS NIGHT DRIVING RECOMMENDED?

 Yes
Yes  No
No
IS MONOVISION EMPLOYED? |
|
|
|
|
|
|
DID YOUR PATIENT RECEIVE BIOPTIC LENS TRAINING? |
||||
By contact lenses |
Yes |
No |
|
|
|
|
|
Yes |
No |
Not Known |
|
By refractive surgery |
Yes |
No |
|
|
|
|
|
|
|||
|
|
|
|
|
DID PATIENT RECEIVE BIOPTIC LENS TRAINING THAT INCLUDED DRIVING? |
||||||
Is best corrected visual acuity in each eye recommended for driving? |
Yes |
No |
Yes |
No |
Not Known |
|
|||||
|
|
|
|
|
|
|
|
|
|
||
Bioptic Telescope |
Right eye 20/ ___________ |
Left eye 20/___________ |
SKILL IN USING BIOPTIC TELESCOPE |
|
|||||||
|
|
|
|
||||||||
Bioptic Telescope suitable for driving? |
Yes |
No |
|
|
|
Satisfactory |
Unsatisfactory |
Not Known |
|||
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
2. VISUAL ACUITY — Complete Clinical Measurement Section. Lenses include contact lenses or glasses.
DMV MEASUREMENT (FOR DMV USE ONLY) |
|
CLINICAL MEASUREMENT (WITHOUT BIOPTIC TELESCOPE) |
||||||
|
|
|
|
|
|
|
|
|
|
Both Eyes |
Right Eye |
|
Left Eye |
|
Both Eyes |
Right Eye |
Left Eye |
|
|
|
|
|
|
|
|
|
Without Lenses |
20/ |
20/ |
|
20/ |
Without Lenses |
20/ |
20/ |
20/ |
|
|
|
|
|
|
|
|
|
With Current Lenses |
20/ |
20/ |
|
20/ |
With Lenses |
20/ |
20/ |
20/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Best Corrected Visual Acuity |
20/ |
20/ |
20/ |
3.DIAGNOSIS — Please indicate vision condition by checking the box(es) representing affected eye(s). If the diagnosed condition is not listed, write the diagnosis under “other diagnosis/comments” below.
REFRACTIVE R L DEVELOPMENTAL
Astigmatism |
Amblyopia |
Hyperopia |
Strabismus |
Myopia |
Congenital Nystagmus |
|
Albinism |
R L OPTICAL |
R L RETINAL/OPTIC NERVE R L |
Cataract |
Diabetic Retinopathy |
Corneal Opacity |
Macular Degeneration |
Diplopia (uncorrectable) |
Glaucoma |
Keratoconus |
Retinal Detachment |
Aphakia |
Retinitis Pigmentosa |
Pseudophakia |
Retinal Damage |
Post. Caps. Opac. |
(CRVO, PRP etc.) |
VISUAL FIELDS |
R L |
Decreased Peripheral Vision |
|
Hemianopia |
|
Quadrantanopia |
|
Decreased Peripheral Vision. Please identify the areasaffectedonthechartinSection5(seereverse)
Other diagnosis/comments
Monocular Vision (No Light Perception or Prosthesis) |
If monocular, when was the monocular vision diagnosed? |
|
|
|||||
If monocular, does the patient have a medical condition that could affect the functional eye in the future? |
Yes |
No |
||||||
Any eye surgery (including refractive)? |
Yes |
No |
Date of most recent surgery |
|
Type of surgery |
|
||
|
|
|
|
|
|
|
|
|
DL 62 (REV. 4/2016) WWW |
*DL62* |
|
Name: |
DL/ID/X #: |
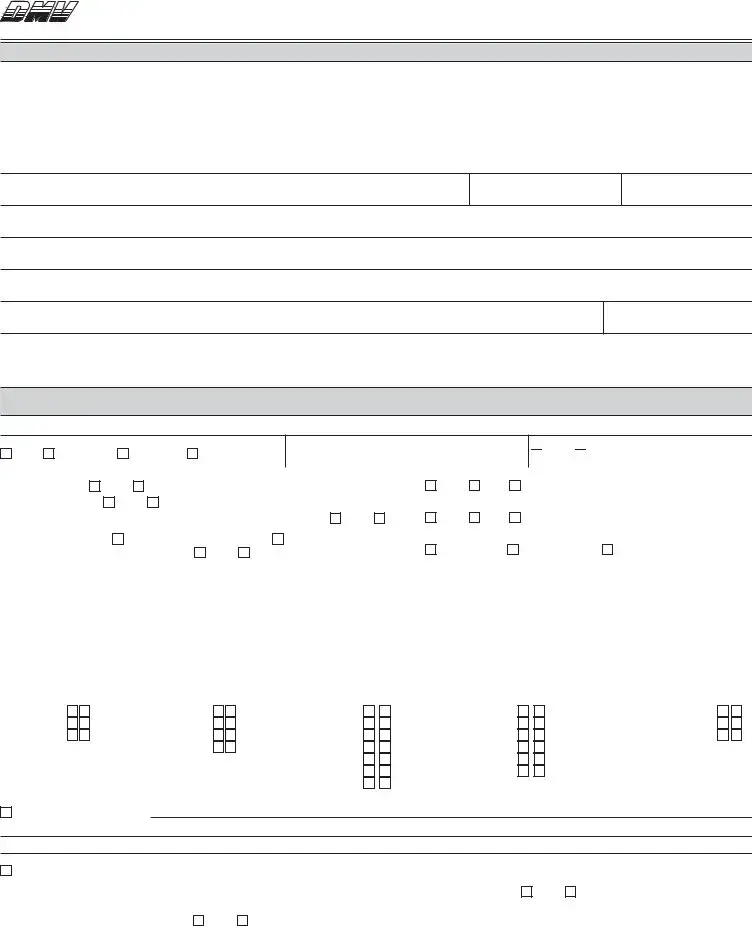
4. PROGNOSIS
Diagnosis |
|
Static |
Diagnosis |
|
Static |
Diagnosis |
|
Static |
Progressive |
Stable since |
|
(date) |
Progressive |
Stable since |
|
(date) |
Progressive |
Stable since |
|
(date) |
WHEN SHOULD DMV REQUIRE A NEW DMV VISION EXAMINATION REPORT FORM BE SUBMITTED?

 Not applicable
Not applicable  1 year
1 year 
 2 years
2 years  5 years
5 years 
 Other
Other
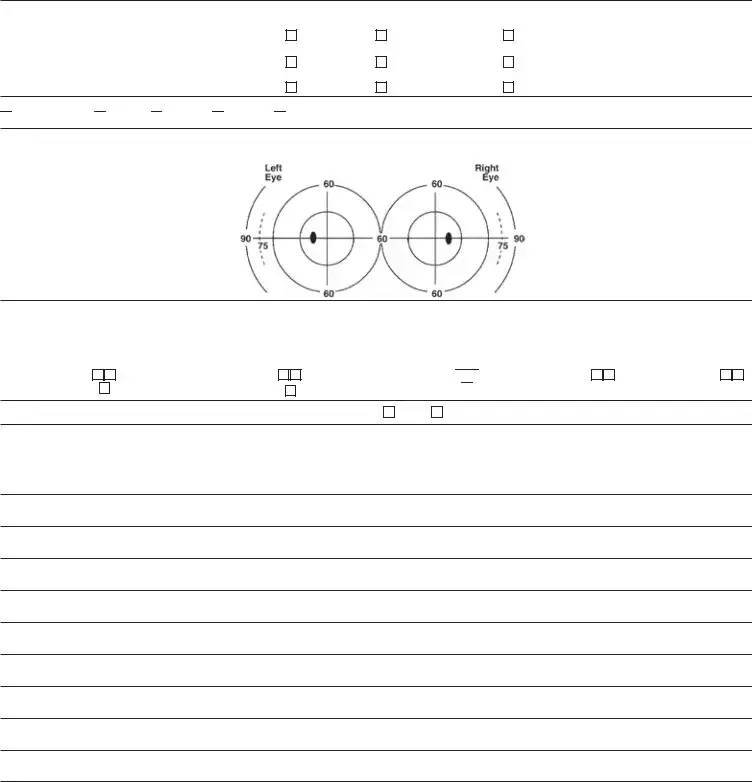
5.VISUAL FIELDS — If vision is not correctable to 20/40 in each eye, or there is possible visual ield loss, a full visual ield examination (con- frontation is permissible) must be performed. Show the approximate peripheral extent and any scotomas in the diagram below.
|
LEFT EYE |
|
RIGHT EYE |
|
Extent: |
|
|
Extent: |
|
Left |
|
|
|
Left |
Right |
|
|
|
Right |
Up |
|
|
|
Up |
Down |
|
|
|
Down |
6.VISUAL ABNORMALITIES — The following information will help our examiners evaluate your patient’s ability to safely operate a motor vehicle. Based upon your testing, clinical impression, or knowledge of the disorder, please indicate the severity of any of the following visual abnormalities which your patient may be experiencing. Indicate severity of condition by placing a 1 (mild), 2 (moderate), or 3 (severe) in the box(es) below.
R L
Decreased Acuity
Color Defect
R L
Visual Field Loss
Reduced Depth Perception
R L
Contrast Sensitivity Loss 
 Abnormal Eye Movements
Abnormal Eye Movements 

R L
Problems With Glare
R L
Poor Night Vision
7. ADVICE — Have you given your patient any advice about driving? |
Yes |
No |
If yes, please explain in #8 below. |
8.ADDITIONAL COMMENTS — Report any additional information or comments you feel DMV should know concerning your patient’s visual and perceptual capabilities relating to driving performance. You may use an additional sheet of paper to provide this information as well as
information about any existing conditions which contribute to poor night vision or poor depth perception, etc. Any recommendations about the patient’s general safety should also be made. DMV will make the inal licensing decision based on a combination of factors, including your professional expertise.
9. SIGNATURE — This section must be completed to validate this report.
PRINTED NAME |
|
|
|
M.D. OR O.D. LICENSE NUMBER |
|
|
|
|
|
|
|
SIGNATURE |
|
|
|
DATE OF EXAM (MUST BE WITHIN LAST 6 MONTHS) |
|
X |
|
|
|
|
|
ADDRESS |
CITY |
CA |
ZIP CODE |
TELEPHONE NUMBER |
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
DL 62 (REV. 4/2016) WWW
Form Data
| Fact | Detail |
|---|---|
| Document Title | 962 Report of Vision Examination |
| Issuing Body | State of California Department of Motor Vehicles (DMV) |
| Confidentiality | All medical information received by DMV is confidential under California Vehicle Code (CVC) §1808.5. |
| Valid Timeframe | The vision examination must have been conducted within the last six months. |
| DMV's Visual Acuity Screening Standard | 20/40 with both eyes tested together, 20/40 in one eye, and at least 20/70 in the other eye. |
| Requirement for Further Examination | If vision is not correctable to 20/40 in each eye, or there is possible visual field loss, a full visual field examination must be performed. |
| Final Licensing Decision | DMV will make the final licensing decision based on a combination of factors, including the vision specialist's provided information. |
Instructions on Utilizing Dmv Vision
Filling out the DMV Vision Form is a critical step in ensuring that your driving capabilities are accurately assessed, particularly if you have vision concerns that could impact your driving. The process is straightforward, but it's important to provide accurate and complete information to avoid any delays in your license issuance or renewal process. Follow these steps to fill out the form correctly.
- Begin with Section 1, which must be completed by the applicant. Here, fill in your driver license number, your date of birth, your home telephone number, and your residence address (including city, state, and ZIP code).
- Next, clearly print your name (first, middle, last) in the spaces provided.
- Read the authorization statement carefully. If you agree, sign your name on the applicant’s signature line and write the current date next to it.
- Proceed to Section 2, which should be completed by your ophthalmologist or optometrist. It's important to note that this information must be from an examination conducted within the last six months.
- In the Refraction subsection, your vision specialist will indicate whether new distance lenses have been prescribed and fitted, and if so, what type (glasses or contact lenses).
- Your specialist will also note recommendations on night driving, the employment of monovision, and whether you have received bioptic lens training.
- In the Visual Acuity subsection, clinical measurements of your vision with and without lenses will be recorded, for both eyes together and each eye individually.
- The Diagnosis section is next, where your vision specialist will check the boxes corresponding to any vision conditions you have. If your condition isn't listed, it can be added under "other diagnosis/comments".
- The Prognosis subsection allows the specialist to indicate whether your vision condition is static or progressive, and when DMV should require a new Vision Examination Report Form to be submitted.
- The Visual Fields section is for documenting peripheral vision extent and any scotomas (blind spots).
- Under Visual Abnormalities, the specialist will rate the severity of any issues such as decreased acuity or problems with glare, which could impact your driving.
- In the Advice section, any suggestions or warnings given to you regarding your driving will be noted.
- The Additional Comments section is for any other information that might help DMV in their evaluation.
- Finally, your vision specialist must complete the signature section at the end of the form, including printed name, M.D. or O.D. license number, signature, date of exam, address, and telephone number.
After completing the form, remember to bring it along with any new corrective lenses to your DMV appointment. Do not mail this form back to DMV unless specifically instructed to do so. Accurate completion and compliance with these steps expedite the evaluation process and contribute to a smoother experience at DMV.
Obtain Answers on Dmv Vision
What is a DMV Vision Form?
The DMV Vision Form, officially known as the "Report of Vision Examination" (DL 62), is a document created by the Department of Motor Vehicles in California. It is used to record the findings of a vision examination conducted by a qualified vision specialist, such as an ophthalmologist or optometrist. The form is part of the process to determine an individual's fitness to safely operate a motor vehicle based on their visual capabilities.
Who needs to complete the DMV Vision Form?
Individuals who are applying for a driver's license or those seeking to renew their license might be required to complete this form if the DMV deems it necessary to assess their vision. It may also be required if there has been a noticeable change in an individual’s vision that could affect their driving abilities.
What sections are included in the DMV Vision Form?
The form is divided into several sections. The first section is to be completed by the applicant, providing personal information and authorization for the vision specialist to share examination results with the DMV. Subsequent sections are filled out by the vision specialist, detailing the results of the vision examination, including assessments of refractive error, visual acuity, diagnosis of any eye conditions, prognosis, visual fields, and other visual abnormalities.
How often does the vision exam need to be conducted?
According to the form, the vision examination should be conducted within the last six months before submitting the form to the DMV. Vision specialists are advised to perform a new vision examination unless one has been conducted in this timeframe.
What are the DMV's vision standards according to the form?
The form specifies that the DMV’s Visual Acuity Screening Standard requires an individual to have 20/40 visual acuity with both eyes tested together, 20/40 in one eye, and at least 20/70 in the other eye to meet the DMV's vision standards for driving.
Can alterations be made to the DMV Vision Form?
Alterations or erased information on the form may void the document. It is crucial that the information provided is accurate and complete to prevent the need for a new vision examination and to ensure the form is valid for DMV's use.
What happens if the form is incomplete?
If any section of this form is incomplete, it may be returned to the vision specialist for completion. This is to ensure that the DMV has all the necessary information to make an informed licensing decision based on the applicant’s visual capabilities.
Should the completed DMV Vision Form be mailed to the DMV?
Applicants are instructed not to mail this form to the DMV unless specifically asked to do so by a DMV employee. Typically, individuals will bring this completed form along with any new corrective lenses to their DMV appointment for further testing or discussion.
Who makes the final licensing decision?
The form states that the DMV will make the final licensing decision based on a combination of factors, including the information from the vision specialist. This underscores the importance of the vision examination and the role of professional expertise in assessing an individual's ability to drive safely.
Common mistakes
Completing the Department of Motor Vehicles (DMV) Vision Exam form is a critical step for individuals in ensuring their ability to drive safely on the roads. However, mistakes during this process can not only delay one's application but can also impact the licensing decision. Below are five common mistakes made when filling out the DMV Vision Exam form:
Leaving Sections Incomplete: One of the most significant errors is not filling out every required section of the form. The DMV stipulates that all parts of the form must be completed for the application to proceed. Failure to provide complete information can result in the form being returned for further details, causing unnecessary delays.
Incorrect Information: Another common mistake is entering incorrect information, particularly in the applicant's personal details section. This includes errors in the driver license number, date of birth, and contact information. Accurate data is crucial for the DMV's records and any misstep here can lead to confusion and misidentification.
Alteration or Erased Information: The DMV explicitly warns against altering or erasing information on the form as it may void the document. Any need to make changes should be addressed by completing a new form to avoid discrepancies that could cast doubt on the validity of the submitted information.
Overlooking the Signature and Date: The applicant’s signature and the date are vital for validating the form. This section authorizes the vision specialist to share the examination results with the DMV. An unsigned form or a form without a date is considered incomplete and cannot be processed.
Failure to Report New Corrective Lenses: If new corrective lenses (glasses or contact lenses) have been prescribed and fitted, this information must be accurately reported on the form. Neglecting to update this information can lead to inaccuracies in the DMV's assessment of an individual's ability to meet the visual acuity standards required for safe driving.
Ensuring the accuracy and completeness of the DMV Vision Exam form is crucial. Applicants must provide precise information and adhere strictly to the instructions to facilitate a smooth process with the DMV. Common errors, such as those listed above, can be easily avoided by taking the time to review the form carefully before submission.
Documents used along the form
Filing the DMV Vision Examination Form is an important step for individuals with visual impairments seeking to obtain or renew their driver’s license. However, this document often accompanies other key forms and documents during the application process, ensuring the Department of Motor Vehicles (DMV) has a comprehensive understanding of the applicant’s ability to safely operate a vehicle. Here are four such documents:
- Medical Examination Report Form (MER): This form provides a detailed report of the applicant’s overall physical health, not just their vision. It must be completed by a certified medical examiner. The form evaluates the applicant’s medical fitness to safely drive a commercial vehicle, but it's sometimes required for non-commercial drivers with certain medical conditions as well.
- Driver’s License Application Form: The essential document for anyone applying for a new, renewal, or replacement driver’s license. It captures basic personal information, driving history, and the type of vehicle the applicant intends to operate.
- Proof of Identity and Residency Documents: Applicants must provide documents such as a birth certificate, passport, or state ID for proof of identity. Additionally, documents like utility bills or lease agreements prove the applicant’s residency within the state.
- Road Test Scheduling Form: For new drivers or drivers whose licenses have been expired or revoked, passing a road test is mandatory. This form is used to schedule a driving test with the DMV. It requires the applicant’s personal information and preferred DMV location for taking the test.
Together, these forms and documents play crucial roles in ensuring that not only the vision but also the overall health, identity, and practical driving skills of the applicant meet the safety standards required to operate a vehicle. By providing a holistic view of the applicant, the DMV can make informed decisions about licensing, thereby contributing to safer roadways for everyone.
Similar forms
Medical Examination Report for Commercial Driver Fitness Determination: This form, often used for commercial driving licenses, shares similarities with the DMV Vision form because it requires detailed health and vision assessments from a healthcare professional to ascertain an individual's fitness to drive. Just like the DMV Vision form, it includes sections for the health professional’s findings, advice on driving ability, and any recommended restrictions or conditions.
Medical Certification for Disability Exceptions (SSA-1020): Used for social security purposes, this document echoes the DMV Vision form in its structure of collecting detailed medical information regarding a person’s physical condition, including vision, which is used to evaluate their eligibility for benefits, paralleling the evaluation of driving capabilities by the DMV.
Flight Physical Examination Form: Required by the Federal Aviation Administration (FAA) for pilots, this form includes comprehensive vision testing similar to the DMV Vision form. Both assess visual acuity, field of vision, and other aspects crucial for safety in their respective fields – driving and flying.
Pre-Employment Physical Examination Forms: Common in many industries, these forms often include a section for vision testing akin to the DMV Vision form, intended to ensure that a candidate’s vision meets the job’s safety requirements, reflecting the DMV’s concern for road safety.
Application for Disability Parking Certificate: This form, used by many states, requires a medical professional’s certification for eligibility, similar to the DMV Vision form. It focuses on how an individual's mobility is affected by their condition, including vision impairments, impacting their need for closer parking access.
Annual Athlete Physical Examination Form: Required for participation in many sports, this form parallels the DMV Vision form through its inclusion of a vision test to ensure an athlete can safely compete, emphasizing the role of good vision in personal safety across different activities.
Life Insurance Medical Examination Form: This form requires a comprehensive health examination, including vision, to determine risk factors, much like the DMV Vision form evaluates vision to assess driving risks, reflecting the integral role of vision in evaluating overall health and safety capabilities.
School Entry Health Exam Certification: Similar to the DMV Vision form's requirement for vision assessment by a professional, this form must be completed for school entry to ensure children meet health standards, including vision, for safe participation in educational activities.
Firearm Ownership Background Check and Mental Health Declaration: Although primarily focused on mental health and criminal background, some versions also require a physical health declaration, including vision, paralleling the DMV Vision form’s emphasis on the importance of vision for safe practices – in this case, relating to the use of firearms.
Diving Fitness Examination Form: Required for scuba diving certifications, this form includes a vision examination to ensure dive safety, similarly acknowledging the critical importance of vision, as does the DMV Vision form in the context of driving safety.
Dos and Don'ts
Filling out the DMV Vision Form is a crucial step in ensuring that drivers meet the visual standards required for safe driving. To assist individuals in completing the form accurately and efficiently, here are essential do's and don'ts to consider:
Do:- Ensure all sections are completed: Before submitting the form, double-check that all required sections are filled out. Incomplete information can lead to delays in processing.
- Report current information: Provide the most up-to-date and accurate information regarding vision and corrective lenses, if applicable.
- Include new corrective lens prescriptions: If new corrective lenses have been prescribed, make sure this is clearly indicated on the form, as it could impact the visual acuity standards required by the DMV.
- Sign and date the form: The applicant's signature is necessary to authorize the vision specialist to release information to the DMV. Ensure that the form is signed and dated before submission.
- Leave sections blank: Avoid submitting the form with incomplete information. Every section that applies to you must be filled out thoroughly.
- Alter or erase information: Making changes or erasing information after it has been entered can void the form. If corrections are needed, it's advisable to start with a fresh form to ensure clarity.
- Mail the form without instruction: Do not mail the form to the DMV unless specifically instructed by a DMV employee. Usually, the form should be brought in person to the DMV office.
- Ignore the need for a recent exam: The DMV requires that the vision examination be conducted within the last six months. Ensure that the examination date is within this timeframe before submitting the form.
Adhering to these guidelines will facilitate a smoother process in meeting the DMV's requirements for visual acuity, ultimately supporting the goal of maintaining safe driving standards.
Misconceptions
When it comes to completing the DMV Vision Examination form, many people hold misconceptions that can lead to unnecessary stress and confusion. Understanding the truth behind these misunderstandings can make the process smoother for everyone involved. Here are nine common misconceptions about the DMV Vision form, explained:
All sections of the form must be filled out by the applicant. Contrary to this belief, only Section 1 requires completion by the applicant. The rest should be filled out by a licensed vision specialist, such as an ophthalmologist or optometrist.
The form must be mailed back to the DMV by the applicant. The instructions clearly state that the form should not be mailed back to the DMV by the applicant unless specifically requested by a DMV employee. Typically, the applicant will bring the completed form back to the DMV for further action.
Any eye care professional can complete the form. Only a licensed ophthalmologist or optometrist is qualified to complete the sections that apply to the vision examination. This ensures the accuracy and reliability of the medical information provided.
The vision test is the sole factor in determining licensing eligibility. While vision is a critical component, the DMV makes licensing decisions based on a combination of factors. This may include other medical conditions, driving tests, and the information provided by the vision specialist.
Once filled out, the form is valid indefinitely. The form must be based on an examination conducted within the last six months. This requirement ensures that the DMV has the most recent and relevant information regarding the applicant's vision.
Corrective lenses prescribed are not significant to the DMV. It's crucial to indicate on the form whether new corrective lenses have been prescribed and fitted, as this can significantly impact visual acuity and, consequently, driving safety.
If you pass the vision test, other vision conditions do not matter. The form includes sections for diagnosing vision conditions and for prognostic information. These sections help the DMV understand the broader context of the applicant's visual health, not just their ability to meet the acuity standard.
Only visual acuity is tested and considered. The form also requires information on visual fields, the presence of visual abnormalities such as color defects or contrast sensitivity loss, and any advice given by the vision specialist regarding driving. This comprehensive approach ensures a holistic evaluation of the applicant’s visual capabilities.
Applicants can decide whether monovision is employed. The use of monovision correction must be revealed in the examination, as it impacts one's depth perception and overall visual function. It’s a critical detail that requires professional assessment and documentation.
Clearing up these misconceptions emphasizes the importance of a thorough and accurate vision assessment. It also underlines the DMV’s commitment to ensuring that all drivers meet the necessary visual standards for safe driving.
Key takeaways
Filling out and using the DMV Vision form is an essential step for individuals needing to report their vision status to the Department of Motor Vehicles, especially when aiming to obtain or renew a driver's license. It involves collaboration between the applicant and a vision specialist. Here are five key takeaways about this process:
- Applicant and Vision Specialist Roles: The form is divided into sections that require both the applicant and an ophthalmologist or optometrist to complete. The applicant fills out the initial part, including personal information and consent, while the vision specialist fills out the detailed vision examination results.
- Recent Examination Requirement: Vision specialists should provide information from an exam conducted within the last six months. This ensures that the DMV receives the most current assessment of the applicant's vision.
- Confidentiality of Information: All medical information supplied to the DMV through this form is confidential, complying with California Vehicle Code §1808.5. Applicants and vision specialists can be assured of the privacy of the disclosed information.
- Importance of Complete and Accurate Information: To avoid delays, all sections of the form must be completely and accurately filled. Incomplete information or alterations to the form can result in it being returned for corrections, which can delay the licensing decision.
- Final Decision by DMV: Even with a detailed vision report from a qualified specialist, the final licensing decision rests with the DMV. They will consider the comprehensive vision examination report among other factors to assess an applicant's ability to safely operate a motor vehicle.
Understanding these key aspects can streamline the process of submitting a DMV Vision form and facilitate a smoother interaction with the Department of Motor Vehicles for vision-related licensing requirements.
Popular PDF Forms
Physician's Statement Disability Form - A formal procedure involving a physician’s insight into a patient’s condition for insurance validation.
Privacy Act Statement for Email - Reinforces the sanctity of personal privacy through stringent handling requirements for documents, as mandated by the Privacy Act of 1974.