Blank Driver Qualification PDF Template
In the realm of commercial driving, thorough vetting and evaluation of drivers to ensure compliance with federal safety standards and regulations is paramount. This is where the Driver Qualification File (DQF) comes into play. It encompasses a comprehensive checklist designed to assess and document a driver's eligibility under the governing standards. Key components of this file include a driver's application for employment, detailing personal, licensure, and historical residence data essential for a background check; inquiries to previous employers and state agencies, capturing a driver's work history and any notable driving infractions; and crucially, the medical examiner's certificate, which is a testament to the driver's health and physical ability to operate commercial vehicles safely. Other significant parts of the DQF include documentation of a driver’s road test performance, annual certification of violations, and a review of the driving record—each serving to cement the driver’s qualifications. Notably, for drivers operating under multiple employers, a specific checklist ensures consistency in qualification standards. This intricate process underscores the importance of rigor and diligence in maintaining road safety and regulatory compliance, highlighting the need for drivers to have immediate access to certain certificates, such as the medical examiner's certificate, while driving.
Preview - Driver Qualification Form
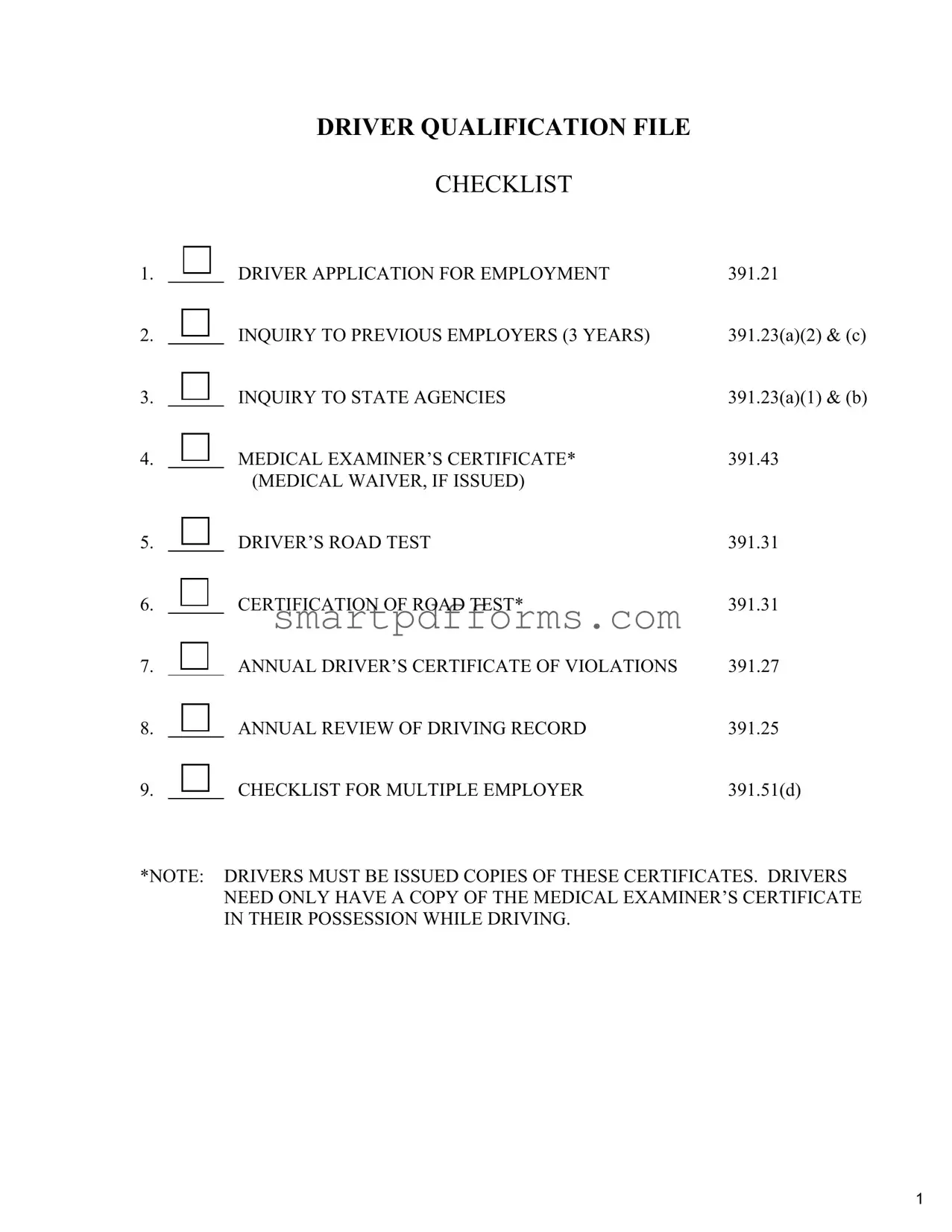
DRIVER QUALIFICATION FILE
CHECKLIST
1. |
|
DRIVER APPLICATION FOR EMPLOYMENT |
391.21 |
2. |
|
INQUIRY TO PREVIOUS EMPLOYERS (3 YEARS) |
391.23(a)(2) & (c) |
3. |
|
INQUIRY TO STATE AGENCIES |
391.23(a)(1) & (b) |
4. |
|
MEDICAL EXAMINER’S CERTIFICATE* |
391.43 |
|
|
(MEDICAL WAIVER, IF ISSUED) |
|
5. |
|
DRIVER’S ROAD TEST |
391.31 |
6. |
|
CERTIFICATION OF ROAD TEST* |
391.31 |
7. |
|
ANNUAL DRIVER’S CERTIFICATE OF VIOLATIONS |
391.27 |
8. |
|
ANNUAL REVIEW OF DRIVING RECORD |
391.25 |
9. |
|
CHECKLIST FOR MULTIPLE EMPLOYER |
391.51(d) |
*NOTE: DRIVERS MUST BE ISSUED COPIES OF THESE CERTIFICATES. DRIVERS NEED ONLY HAVE A COPY OF THE MEDICAL EXAMINER’S CERTIFICATE IN THEIR POSSESSION WHILE DRIVING.
1
(enter company name)
(enter address)
__________________
(enter phone number)
COMMERCIAL DRIVER APPLICATION
FILL IN ALL BLANKS & PROVIDE ALL INFORMATION
…………………………………………………………………………………………………………………………………….
Date: _______________________
Name: |
First_____________________ Middle_________________ Last______________________________________ |
|||
Address _________________________________________________ |
|
Home telephone: _____________________ |
||
City_______________________ State _______ Zip ___________ |
Cellular telephone: _____________________ |
|||
Date of Birth: ____________________________ |
Social Security Number: _______ - _______ - __________ |
|||
|
||||
|
|
|
|
|
If your above address is less than 3 years continue listing them below to cover the previous 3 year period: |
||||
1 |
Street_________________________________________________ |
Dates: From_________ To_________ |
||
City_______________________ State _______ Zip ___________
……………………………………………………………………………………………………………………………….
2 Street_________________________________________________ Dates: From_________ To_________
City_______________________ State _______ Zip ___________
……………………………………………………………………………………………………………………………….
3 |
Street_________________________________________________ |
Dates: From_________ To_________ |
|
City_______________________ State _______ Zip ___________ |
|
|
Use backside of sheet for additional addresses |
|
Driver’s License Information: all licenses held, last 3 years:
State_______________ Number___________________________________________ Expiration Date _______________
State_______________ Number___________________________________________ Expiration Date _______________
State_______________ Number___________________________________________ Expiration Date _______________
Experience: |
|
|
__________________________________ |
________________ to ________________ |
____________________________ |
Type of vehicle driven |
Dates |
Approximate mileage driven |
__________________________________ |
________________ to ________________ |
____________________________ |
Type of vehicle driven |
Dates |
Approximate mileage driven |
__________________________________ |
________________ to ________________ |
____________________________ |
Type of vehicle driven |
Dates |
Approximate mileage driven |
All Accidents, last 3 years: (If none, write NONE)
Date________________ Describe_______________________________ Fatalities_____________ Injuries_____________
Date________________ Describe_______________________________ Fatalities_____________ Injuries_____________
Date________________ Describe_______________________________ Fatalities_____________ Injuries_____________
July2003,dlnm2
revised 08/04
List all Traffic Violations Convictions, last 3 years: (If none, write NONE) |
|
|
|
|
||||
Date______________ Violation____________________________________ State_______ Commercial Vehicle: Yes / No |
|
|||||||
Date______________ Violation____________________________________ State_______ Commercial Vehicle: Yes / No |
|
|||||||
Date______________ Violation____________________________________ State_______ Commercial Vehicle: Yes / No |
|
|||||||
Date______________ Violation____________________________________ State_______ Commercial Vehicle: Yes / No |
|
|||||||
Date______________ Violation____________________________________ State_______ Commercial Vehicle: Yes / No |
|
|||||||
Date______________ Violation____________________________________ State_______ Commercial Vehicle: Yes / No |
|
|||||||
Date______________ Violation____________________________________ State_______ Commercial Vehicle: Yes / No |
|
|||||||
Date______________ Violation____________________________________ State_______ Commercial Vehicle: Yes / No |
|
|||||||
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
Have you ever had any driver license denied, suspended, revoked or canceled by any issuing state agency? |
|
|
|
|||||
|
Yes |
No |
If yes; state of issuance; explanation: ___________________________________________________ |
|
||||
____________________________________________________________________________________________________ |
|
|
||||||
|
|
|||||||
|
|
|
|
|
|
|
|
|
Employment History, last 10 years |
|
|||||||
1) |
Employer:_____________________________________________ |
Dates: ________________to________________ |
|
|||||
|
Address: _____________________________________________ |
Supervisor: ______________________________ |
|
|||||
|
City, State, Zip code:____________________________________ |
Telephone: ______________________________ |
|
|||||
Were you subject to the Federal Motor Carrier Safety Regulations during this period? |
Yes |
No |
|
|||||
Were you subject to 49 CFR part 40 controlled substance and alcohol testing during this period? |
Yes |
No |
|
|||||
Reason for Leaving: __________________________________________________________________________________ |
|
|||||||
____________________________________________________________________________________________________ |
|
|
||||||
|
|
|
||||||
………………………………………………………………….……………………….………………………………………... |
|
|||||||
2) |
Employer:_____________________________________________ |
Dates: ________________to________________ |
|
|||||
|
Address: ___________________________________________ Supervisor:________________________________ |
|
||||||
|
City, State, Zip code: ____________________________________ |
Telephone: ______________________________ |
|
|||||
Were you subject to the Federal Motor Carrier Safety Regulations during this period? |
Yes |
No |
|
|||||
Were you subject to 49 CFR part 40 controlled substance and alcohol testing during this period? |
Yes |
No |
|
|||||
Reason for Leaving: __________________________________________________________________________________ |
|
|||||||
____________________________________________________________________________________________________ |
|
|
||||||
………………………………………………………………….……………………….………………………………………... |
|
|||||||
|
|
|
|
|
|
July2003,dlnm |
3 |
|
|
|
|
|
|
|
revised 08/04 |
||

3)Employer:_____________________________________________ Dates: ________________to________________
Address: _____________________________________________ Supervisor: ______________________________
City, State, Zip code: _____________________________________Telephone: ______________________________
Were you subject to the Federal Motor Carrier Safety Regulations during this period? |
Yes |
No |
Were you subject to 49 CFR part 40 controlled substance and alcohol testing during this period? |
Yes |
No |
Reason for Leaving: __________________________________________________________________________________
____________________________________________________________________________________________________
………………………………………………………………….……………………….………………………………………...
4)Employer:_____________________________________________ Dates: ________________to________________
Address: _____________________________________________ Supervisor:________________________________
City, State, Zip code______________________________________ Telephone: ______________________________
Were you subject to the Federal Motor Carrier Safety Regulations during this period? |
Yes |
No |
Were you subject to 49 CFR part 40 controlled substance and alcohol testing during this period? |
Yes |
No |
Reason for Leaving: __________________________________________________________________________________
____________________________________________________________________________________________________
………………………………………………………………….……………………….………………………………………...
5)Employer:_____________________________________________ Dates: ________________to________________
Address: _____________________________________________ Supervisor: ______________________________
City, State, Zip code:_____________________________________ Telephone: ______________________________
Were you subject to the Federal Motor Carrier Safety Regulations during this period? |
Yes |
No |
Were you subject to 49 CFR part 40 controlled substance and alcohol testing during this period? |
Yes |
No |
Reason for Leaving: __________________________________________________________________________________
____________________________________________________________________________________________________
………………………………………………………………….……………………….………………………………………...
6) Employer:_____________________________________________ Dates: ________________to________________
Address: _____________________________________________ Supervisor: ______________________________
City, State, Zip Code:_____________________________________Telephone: ______________________________
Were you subject to the Federal Motor Carrier Safety Regulations during this period? |
Yes |
No |
Were you subject to 49 CFR part 40 controlled substance and alcohol testing during this period? |
Yes |
No |
Reason for Leaving: __________________________________________________________________________________
____________________________________________________________________________________________________
………………………………………………………………….……………………….………………………………………...
revised 08/04 |
4 |
|
|
July2003,dlnm |
|
7) Employer:_____________________________________________ Dates: ________________to________________
Address: _____________________________________________ Supervisor: ______________________________
City, State, Zip code:_____________________________________ Telephone: ______________________________
Were you subject to the Federal Motor Carrier Safety Regulations during this period? |
Yes |
No |
Were you subject to 49 CFR part 40 controlled substance and alcohol testing during this period? |
Yes |
No |
Reason for Leaving: __________________________________________________________________________________
____________________________________________________________________________________________________
Use backside of sheet for additional employers
For driver applicants of commercial motor vehicles that require a Commercial Driver License (CDL) the applicant must disclose their controlled substance and alcohol status per the requirements of 49 CFR part 40.25(j).
As a prospective driver employee, you have the right to review information provided by previous employers. You have the right to have errors in the information corrected by the previous employer(s) and for that previous employer(s) to re
Driver employees who have previous Department of Transportation regulated employment history in the preceding three years, and wish to review previous employer provided investigative information, must submit a written request to the prospective employer, which may be done at anytime, including when applying or as late as thirty (30) days after being employed or being notified of denial of employment. The prospective employer must provide this information to the applicant within five (5) business days of receiving the written request. If the prospective employer has not yet received the requested information from the previous employer(s), then the five (5) business day deadlines will begin when the prospective employer receives the requested safety performance history information. If the driver has not arranged to pick up or receive the requested records within thirty (30) days of the prospective employer making them available, the prospective motor carrier may consider the driver to have waived their request to review the records.
Certification
“I certify that this application was completed by me, and that all entries on it and information in it are true and complete to the best of my knowledge.”
___________________________________________________________ |
__________________________________ |
|||
Applicant’s Signature |
|
Date Signed |
|
|
|
|
|
|
|
|
|
|
|
|
TO BE COMPLETED BY THE EMPLOYER: |
|
|
|
|
Application received by: |
|
Application reviewed for completeness by: |
||
______________________________________________ |
______________________________________________ |
|||
Name |
|
Name |
|
|
_________________________ |
_______________ |
__________________________ |
_______________ |
|
Title |
Date |
Title |
|
Date |
|
|
|
|
|
|
|
|
|
|
SIGNIFICANT DATES: |
Date of Hire: |
|
_____________________________________ |
|
|
|
|||
|
Time & Date of |
|
_____________________________________ |
|
|
Time & Date of |
_____________________________________ |
||
|
Date First Used in Safety Sensitive Position: |
_____________________________________ |
||
|
Date of Termination: |
|
_____________________________________ |
|
revised 08/04 |
5 |
July2003,dlnm |
(enter company name)
___________________________
(enter address)
__________________
(enter phone number)
COMMERCIAL VEHICLE DRIVER APPLICANT
Controlled Substance and Alcohol Questionnaire
Pursuant to 49 CFR part 40.25(j)
…………………………………………………………………………………………………………………………………….
|
Application Date _______________________ |
|
|
|
|
|
|||
|
Name ______________________ |
_______________________ |
______________________________________ |
|
|||||
|
First |
|
|
Middle |
|
Last |
|
|
|
|
Address _________________________________________________ |
Home Telephone |
_____________________ |
|
|||||
|
City_______________________ State _______ Zip ___________ |
Cell Telephone |
_____________________ |
|
|||||
|
Date of Birth |
____________________________ |
Social Security Number ________ - ________ - ________ |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
49 CFR 40.25(j) |
|
|
|
|
|
|
|
|
|
|
||||
|
Have you ever tested positive, or refused to test, on any pre |
|
|
|
|||||
|
drug or alcohol test administered by an employer to which you applied |
YES |
NO |
|
|||||
|
for, but did not obtain, |
|
|||||||
|
|
|
|
||||||
|
DOT agency drug and alcohol testing rules during the past two years? |
|
|
|
|||||
|
|
|
|
|
|
|
|||
|
If YES — |
|
Have you successfully completed the |
YES |
NO |
|
|||
|
|
process? |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
Documentation MUST BE PROVIDED before any |
|
|||||
|
If YES — |
|
transportation function is performed. |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
___________________________________________________________ |
__________________________________ |
Applicant’s Signature |
Date Signed |
TO BE COMPLETED BY EMPLOYER:
………………………………………………………………….……………………….………………………………………...
______________________________________________ |
______________________________________________ |
||
Received by: |
|
Reviewed by: |
|
____________________ |
_______________ |
____________________ |
_______________ |
Title: |
Date: |
Title: |
Date: |
July2003,dlnm |
6 |
revised 08/04 |
|
The Federal Motor Carrier Safety Regulations require all previous employers of this applicant to respond to this request for information within 30 days. Failure to comply with this request is in violation of 49CFR 391.23 and 40.25, for which you may be prosecuted. Questions concerning the requirements of this regulation should be directed to the Minnesota Division Office of the Federal Motor Carrier Safety Administration at
TO: |
(enter former employer's name) |
|
________________________________________________ DATE: _________________ |
||
|
Former Employer’s Name |
|
|
(enter mailing address) |
|
|
Mailing Address |
|
|
(enter city / state / zip) |
|
|
City / State / Zip |
|
|
_____________________ |
(enter fax number) |
|
Telephone # |
Fax Number |
(enter name)
I, ______________________________, hereby authorize ___________________________ to release to all records of
employment, including assessments of my job performance, ability, and fitness, including the dates of any and all alcohol or drug tests, with confirmed results, and/or my refusal to submit to any alcohol and drug tests and any
rehabilitation completion under direction of Substance Abuse Professional (SAP) and/or Medical Review Officer (MRO) to each and every company (or their authorized agents) making such request in connection with my application for employment with said company. I, hereby, release the above named company, and its employees, officers, directors, and agents from any and all liability of any type as a result of providing the following information to the below mentioned person and/or company.
Applicant’s Signature & Date |
_______________________________ |
___________________ |
|
Witness’s Signature & Date |
_______________________________ |
___________________ |
|
|
|
|
|
REQUEST FROM: |
(enter company name) |
||
Company: |
|||
_______________________________________________________ |
|||
Address/City/State/Zip: |
_______________________________________________________ |
||
Telephone Number: |
(enter phone number) Fax Number: (enter fax number) |
||
Contact Person & Title |
_________________________________ |
_____________________ |
|
NAME OF APPLICANT: |
_________________________________ SSN _________________ |
||
JOB APPLYING FOR: |
_______________________________________________________ |
||
INQUIRY INTO EMPLOYMENT HISTORY, PRECEDING 3 YEARS
•Did applicant work for you as a ____________________________ from ____/____/____ to ____/____/____ YES or NO IF NO, please explain:
_______________________________________________________________________________
•If employed as driver, please answer the following: Company Driver? ______ Owner/Operator? ______ Other? ______
Type of truck(s) and/or truck/tractor(s) operated: ______________________________________________________
Commodities transported: ____________________________ Area of operations: ____________________________
• Accidents? YES or NO IF YES, please give date(s) and brief description of each accident:
__________________________________________________________________________________________
•Why did this employee leave your company?
__________________________________________________________________________________________
• Would you
__________________________________________________________________________________________
•Additional comments:
__________________________________________________________________________________________
INQUIRY FOR ALCOHOL AND CONTROLLED SUBSTANCES INFORMATION, PRECEDING 2 YEARS
• |
|
|
|
|
Alcohol tests with a result of 0.04 or greater? ………. |
YES or NO |
If yes, please give date(s): ________________ |
||
• Verified positive controlled substances test results? … |
YES or NO |
If yes, please give date(s): ________________ |
||
• Refusals to be tested? ………………………………… |
YES or NO |
If yes, please give date(s): ________________ |
||
• |
Was rehabilitation completed as required? …………... |
YES or NO |
If yes, please give date(s): ________________ |
|
Person providing the above information:
Name: ________________________________________________ Title: ______________________________
Company: ________________________________________________ Date: ______________________________
revised 08/04 |
7 |
(enter employer
name and
information
here)
Driver's Name
Driver's Operators Lic. No.
Driver's Social Sec. No.
Dear
The above listed individual has made application with us for employment as a driver. Applicant has indicated that the above numbered operator's license or permit has been issued by your State to applicant and that it is in good standing.
In accordance with Section 391.23(a)(1) and (b) of the Federal Motor Carrier Safety Regulations, we are required to make inquiry into the driving record during the preceding 3 years of every State in which an
Therefore, please certify to us what the individual's driving record is for the preceding 3 years, or certify that no record exists if that be the case.
In the event that this inquiry does not satisfy your requirements for making such inquiries, please send us such forms of yours as are necessary for us to complete our inquiry into the driving record of this individual.
Respectfully yours,
(printed) name of person making inquiry
Title of person making inquiry
(enter company name)
Motor Carrier Name
(enter address)
Street |
City |
State |
Zip |
revised |
08/04 |
8 |

MEDICAL EXAMINER’S CERTIFICATE
I certify that I have examined ______________________________ in accordance with the Federal Motor Carrier Safety
Regulations (49 CFR
only when: |
|
wearing corrective lenses |
driving within an exempt intracity zone (49 CFR 391.62) |
wearing hearing aid |
accompanied by a Skill Performance Evaluation Certificate (SPE) |
accompanied by a ____________waiver/exemption |
qualified by operation of 49 CFR 391.64 |
The information I have provided regarding the physical examination is true and complete. A complete examination form with any attachment embodies my findings completely and correctly, and is on file in my office.
Signature of Medical Examiner |
|
Telephone |
|
|
Date |
|
|
|
|
|
|
|
|
Medical Examiner’s Name (Print) |
|
MD |
DO |
Chiropractor |
||
|
|
|
Physician |
|
Advanced |
|
|
|
|
Assistant |
|
Practice Nurse |
|
Medical Examiner’s License or Certificate No. / Issuing State |
|
|
|
|
||
|
|
|
|
|
|
|
Signature of Driver |
|
|
Driver’s License No. |
|
State |
|
|
|
PLE |
|
|
||
|
|
M |
|
|
|
|
Address of Driver |
|
|
|
|
|
|
|
|
|
|
|
||
Medical Certificate Expiration Date |
|
|
|
|
||
|
SA |
|
|
|
|
|
9
DRIVER’S ROAD TEST EXAMINATION
Driver’s Name: _______________________________________________________________________
Driver’s Address: _____________________________________________________________________
City: ________________________________________ State: ______________ Zip: _______________
The road test shall be given by the motor carrier or a person designated by it. However, a driver who is a motor carrier must be given the test by another person. The test shall be given by a person who is competent to evaluate and determine whether the person who takes the test has demonstrated that he or she is capable of operating the vehicle and associated equipment that the motor carrier intends to assign.
Rating of Performance |
|
__________________ |
The |
__________________ |
Coupling and uncoupling of combination units, if the equipment he or she |
|
may drive includes combination units. |
__________________ |
Placing the equipment in operation. |
__________________ |
Use of vehicle’s controls and emergency equipment. |
__________________ |
Operating the vehicle in traffic and while passing other vehicles. |
__________________ |
Turning the vehicle. |
__________________ |
Braking and slowing the vehicle by means other than braking. |
__________________ |
Backing and parking the vehicle. |
__________________ |
Other, explain: _______________________________________________ |
Type of equipment used in giving the test: _________________________________________________
Examiner’s signature: _____________________________________ Date: ______________________
Remarks:
If the road test is successfully completed, the person who gave it shall complete a certificate of driver’s road test.
10
Form Data
| Fact | Description |
|---|---|
| Content Category | The Driver Qualification File includes essential documentation such as employment application, previous employer inquiries, state agency inquiries, medical certificates, road test certifications, and records of violations and employment history. |
| Governing Regulations | Specific sections of the Federal Motor Carrier Safety Regulations (FMCSRs), including 391.21, 391.23, 391.27, 391.31, 391.43, and 391.51, define the requirements for the content and maintenance of the Driver Qualification File. |
| Purpose | The purpose of the Driver Qualification File is to ensure that drivers meet the Federal qualifications and standards for commercial driving to enhance road safety. |
| Accessibility | Drivers are required to possess a copy of their Medical Examiner’s Certificate while driving, but must also have other documents, such as road test certificates, accessible within their qualification files as per FMCSA regulations. |
Instructions on Utilizing Driver Qualification
Completing the Driver Qualification Form is a crucial step to ensure compliance with transportation regulations and standards. This documentation process assists in verifying that a driver meets all necessary criteria for the job at hand. Careful attention must be paid to each section to accurately capture the applicant’s qualifications, driving history, and any related experiences. Here’s a clear, step-by-step guide to filling out the form:
- Start with entering the company’s name, address, and phone number at the top of the form.
- Fill in the date of application.
- Provide the applicant’s name (first, middle, last) and contact details, including addresses for the past three years if the current address is less than three years old.
- Enter date of birth, social security number, and driver's license information for the last three years, including state, number, and expiration date.
- Detail the experience, specifying the type of vehicle driven, dates, and approximate mileage driven for each listed experience.
- List all accidents in the last three years, including dates, descriptions, fatalities, and injuries. If none, write "NONE".
- Disclose traffic violations convictions for the last three years, indicating the date, violation, state, and if it involved a commercial vehicle. If none, write "NONE".
- Answer whether any driver license was ever denied, suspended, revoked, or canceled, providing details if applicable.
- Fill out employment history for the last ten years, including employer's name, address, dates of employment, supervisor, telephone number, whether subject to Federal Motor Carrier Safety Regulations, and reason for leaving.
- If applicable, disclose controlled substance and alcohol status as per the requirements of 49 CFR part 40.25(j).
- Read the certification statement, then have the applicant sign and print their name, followed by the date signed.
- Finally, the employer section must be completed, recording who received and reviewed the application, including titles and dates.
Upon completion, this form becomes a component of the driver's qualification file, serving as a comprehensive record of the driver’s credentials and history. It is essential for employers to keep this document updated and to review it periodically to ensure ongoing compliance with road safety regulations.
Obtain Answers on Driver Qualification
Frequently asked questions about the Driver Qualification Form can help both employers and drivers navigate through the essential compliance requirements set by the Federal Motor Carrier Safety Regulations (FMCSRs). Understanding these aspects is crucial for maintaining a lawful and efficient operation. Here are some of the most common inquiries:
- What is a Driver Qualification File?
- Which documents are required in a Driver Qualification File?
- Driver's Application for Employment
- Inquiries to Previous Employers (3 years)
- Inquiries to State Agencies (3 years)
- Medical Examiner’s Certificate and Medical Waiver (if issued)
- Driver’s Road Test and Certification
- Annual Driver’s Certificate of Violations
- Annual Review of Driving Record
- Checklist for Multiple Employer Drivers
- What is the purpose of the Driver's Application for Employment?
- Are there any exemptions to who needs a Driver Qualification File?
- How often do the medical examination and certification need to be renewed?
- What happens if a driver has a traffic violation?
- Can a driver see their Driver Qualification File?
- How long must Driver Qualification Files be kept?
A Driver Qualification File (DQF) is a set of documents that motor carriers are required to maintain for each driver they employ, as mandated by the Department of Transportation (DOT). These files are designed to ensure that drivers meet federal regulations for driving commercial vehicles, focusing on safety and compliance.
The required documents include:
Note that drivers are required to have a copy of their Medical Examiner’s Certificate when driving.
This document collects thorough personal, license, and employment history from the driver. It serves as a baseline for verifying that the applicant meets the job qualifications, including their driving history, experience, and any incidents on the road.
Yes, there are exemptions based on the type of transportation, cargo, and the commercial vehicle's operating radius from the business location. However, most drivers operating vehicles over a certain weight, transporting hazardous materials, or carrying a specified number of passengers are required to have a complete DQF.
Drivers must undergo a physical examination by a DOT-certified medical examiner at least every 24 months. Some drivers may be required to get examined more frequently if the medical examiner deems it necessary due to medical conditions.
The driver is required to notify the employer of any traffic violations (excluding parking tickets) within 30 days. Annual reviews are also conducted to ensure compliance, and these violations are recorded in the DQF.
Yes, drivers have the right to review their files. They may request this from their employer, who must provide access within a reasonable period. If there are any inaccuracies, the driver can request corrections or provide a rebuttal.
Employers must maintain the DQF for as long as the driver is employed and for three years after. This ensures that records are available for audits, investigations, or legal proceedings if needed.
Understanding and complying with the requirements for Driver Qualification Files are critical for ensuring the safety of commercial driving operations and adhering to federal regulations.
Common mistakes
Filling out the Driver Qualification form accurately is crucial for compliance and safety. However, applicants often make errors that can affect their employment eligibility. Here are four common mistakes:
Not providing complete address history: Applicants are required to list all addresses where they have lived over the past three years. Sometimes, people leave out parts of their address history or do not provide the complete date range for each address. This omission can lead to an incomplete background check, hindering the application process.
Omitting previous employment details: The form requires a detailed employment history for the last 10 years, including gaps between jobs. Frequently, applicants will miss listing certain employers or fail to account for periods of unemployment. This oversight can raise questions about the applicant's work history and reliability.
Forgetting to mention driving incidents: Applicants must list all accidents and traffic violations within the last three years. Sometimes, individuals mistakenly believe minor incidents or tickets do not need to be reported. However, failing to disclose these details can be seen as falsifying the application, leading to potential disqualification.
Incomplete signature and date sections: Every part of the application needs to be correctly signed and dated, including the certification at the end. An application that is not signed or incorrectly dated is considered incomplete and can delay the hiring process or result in the application being set aside.
Ensuring these common mistakes are avoided can streamline the qualification process and improve an applicant’s chances of being successfully hired.
Documents used along the form
When the process of driver qualification is underway, the Driver Qualification form plays a foundational role. However, to paint a complete picture of a driver's qualifications and ensure compliance with regulatory standards, several other documents are frequently employed alongside this pivotal form. Each serves a distinct purpose, contributing to a thorough evaluation and maintaining the integrity of the driver qualification process.
- Motor Vehicle Record (MVR): The MVR is an essential document that provides a detailed history of the driver’s driving record, including any violations, suspensions, or other infractions. This record helps employers assess the driver’s safety and compliance on the road over a certain period, typically the previous three to five years.
- Pre-Employment Screening Program (PSP) Report: The PSP report offers insight into a driver's roadside inspection and crash history, as per Federal Motor Carrier Safety Administration (FMCSA) records. This document is invaluable for employers in making well-informed hiring decisions by evaluating potential safety risks.
- Drug and Alcohol Testing Records: These records are crucial for verifying that a driver meets the FMCSA’s requirements regarding drug and alcohol use. Employers must maintain records of any tests conducted, including pre-employment screening, random testing, and tests carried out following accidents.
- Previous Employment Verifications: Verification of a driver’s previous employment is necessary to confirm their experience and history with other employers. This includes checking references, reasons for leaving previous positions, and any issues or disciplinary actions taken during the driver's previous employment.
Together with the Driver Qualification form, these documents create a comprehensive profile of each driver, ensuring that only the most qualified and reliable individuals are behind the wheel. This not only complies with regulatory requirements but also promotes safety on the roadways, protecting the driver, the employer, and the general public.
Similar forms
An Employment Application is similar to the Driver Application for Employment section of the Driver Qualification Form. Both collect detailed personal information about the applicant, including past employment history, albeit the Driver Application also specifically requests information pertinent to driving qualifications.
The Previous Employment Verification Form aligns with the Inquiry to Previous Employers. Both are designed to verify an applicant's employment history and job performance from past employers, focusing on ensuring the prospective employee meets the job's requirements.
A Background Check Authorization Form mirrors the Inquiry to State Agencies section, as both authorize the review of the applicant's records held by public bodies. This scrutiny helps ensure the applicant has a compliant history with state regulations relevant to their future job responsibilities.
The Medical Examination Report Form for commercial drivers is akin to the Medical Examiner’s Certificate section. Each form is necessary to certify that the applicant is physically capable of meeting the demands of the position, specifically focusing on their ability to safely operate a commercial vehicle.
A Driver's Road Test or similar practical assessment tools are used in various fields to evaluate an individual's skills directly related to the job, much like the Driver’s Road Test and Certification of Road Test sections assess a commercial driver's capability to operate a vehicle safely.
An Annual Performance Review Form is reminiscent of the Annual Driver’s Certificate of Violations and Annual Review of Driving Record sections. They both aim to regularly assess the individual's performance and compliance with rules, specific to maintaining a high standard of driving for the latter.
The Drug and Alcohol Testing Consent Form reflects the need for controlled substance and alcohol testing in compliance with specific Federal Motor Carrier Safety Regulations, similar to the acknowledgment in the Driver Qualification Form that a driver was subject to such testing in previous employment.
A Multi-Employer History File Checklist is similar to the Checklist for Multiple Employer. Both are used to organize and document an individual's employment history when they have worked for multiple employers within a specified period, ensuring all necessary verifications for compliance and qualifications are managed and recorded.
Dos and Don'ts
Filling out a Driver Qualification form is a critical step in ensuring that drivers meet the necessary standards for safety and compliance. Here are five things you should do and five things you shouldn't do when completing this form:
Do's:
- Ensure accuracy: Double-check all the information provided for accuracy. Mistakes on the form can lead to delays or even disqualification.
- Complete all sections: Don't leave any section blank. If a section doesn't apply, indicate this appropriately with "N/A" or a similar notation.
- Include all relevant employment history: The last 10 years of employment history must be accurately documented, including any gaps in employment.
- Provide detailed accident and violation information: List all accidents and traffic violations within the specified period. Being transparent and accurate is crucial.
- Review and certify: Before submitting, review the entire form to ensure completeness and accuracy. Signing the certification section confirms that all information is true to the best of your knowledge.
Don'ts:
- Avoid guessing: If you are unsure about specific details, such as dates or addresses, take the time to verify them before filling them in.
- Skip sections: Even if you believe a section is not relevant to you, don't skip it. This can be seen as failing to complete the application fully.
- Use unclear handwriting: If you are filling out the form by hand, make sure all information is legible. Illegible forms may be rejected.
- Forget to list all driver licenses: All licenses held within the last three years, including those from other states, must be listed.
- Ignore the importance of accuracy for previous employer inquiries: When providing information for inquiries to previous employers, accuracy is key to ensuring a smooth verification process.
Misconceptions
When it comes to navigating the requirements for drivers within commercial operations, the Driver Qualification (DQ) file is a critical element that often finds itself swathed in misconceptions. As a foundational aspect of compliance under the Federal Motor Carrier Safety Regulations (FMCSRs), it's imperative to clear up these confusions for both employers and potential driver employees. Here are four common misunderstandings about the Driver Qualification form and its components:
Misconception #1: Only commercial driving experience is relevant. While it's true the form places a significant emphasis on commercial vehicle operation, all driving experience can potentially be relevant. This includes personal vehicle operation, which may provide valuable insight into the driver's overall experience and habits on the road.
Misconception #2: Medical examinations are a one-time requirement. Actually, the Medical Examiner’s Certificate is part of an ongoing requirement where drivers must undergo periodic medical examinations to ensure they remain physically qualified to drive. This is not merely a box to be ticked upon initial employment but a recurring part of the driver's qualification file maintenance.
Misconception #3: Employment history inquiries are optional. This couldn't be farther from the truth. Regulations mandate that inquiries to previous employers (covering a period of three years) must be conducted to assess the driver’s safety performance and history. This isn’t a discretionary step; it's a vital aspect of the driver qualification process.
Misconception #4: The Driver Qualification file is solely the responsibility of the driver. While drivers indeed need to provide accurate and comprehensive information, the maintenance and verification of the Driver Qualification file is a shared responsibility. Employers must ensure that the file is complete and updated according to FMCSA regulations. Both parties play a critical role in maintaining compliance.
Understanding these key facets of the Driver Qualification form not only aids in achieving regulatory compliance but also supports the overarching goal of ensuring safety on the roads. Dispelling myths and misconceptions is a step towards fostering a culture of transparency and responsibility within the commercial driving sector.
Key takeaways
Filling out a Driver Qualification form is a critical process for ensuring that individuals who are applying to become commercial drivers meet all the necessary standards and regulations. Here are nine key takeaways to remember:
- Complete the driver application for employment thoroughly. This step is foundational and requires accurate entry of personal information, employment history, and driving experience.
Inquiries to previous employers and state agencies are mandatory.
These steps, covering the last three years, help verify a candidate's driving history and employment record, ensuring compliance with safety standards.A valid Medical Examiner's Certificate is a must-have, sometimes accompanied by a medical waiver if issued. This certifies that the driver is medically fit for duty.
Successfully passing the Driver's Road Test, and obtaining the Certification of Road Test, is crucial. These ensure the driver has the practical skills needed for the job.
Annual documentation is required. This includes the Driver's Certificate of Violations and the Annual Review of Driving Record, which help monitor the driver's ongoing qualification and compliance.
For drivers with multiple employers, a specific checklist must be maintained to organize and track the distinct employment and qualification records.
It's essential for drivers to be issued copies of certain certificates, notably the Medical Examiner’s Certificate and the Certification of Road Test, and to have the Medical Examiner's Certificate in their possession while driving.
Driver applicants need to disclose detailed personal, employment, and driving history over specific periods, including all licenses held in the past three years, any accidents, and all traffic violation convictions.
Prospective drivers have the right to review, correct, or rebut information provided by previous employers per the guidelines of the Department of Transportation. This ensures fairness and accuracy in the qualification process.
Filling out a Driver Qualification form is not just a matter of ticking boxes but a comprehensive process that ensures the safety, reliability, and compliance of commercial drivers. By carefully completing this process, employers and drivers alike contribute to safer roads and more dependable transportation services.
Popular PDF Forms
Form I-765 - Details about the applicant’s last arrival in the U.S. are required on Form I-765.
Idaho Re 21 - Stipulates occupancy intentions of the buyer, which can influence loan terms and insurance policies.