Blank Dwc 73 PDF Template
In the state of Texas, employees who suffer work-related injuries or illnesses are navigated through a process that involves reporting their condition and seeking necessary medical and income benefits with the guidance of the Texas Department of Insurance, Division of Workers’ Compensation (DWC). A crucial document in this process is the DWC 73 form, officially known as the Texas Workers’ Compensation Work Status Report. This form serves multiple purposes including, but not limited to, reporting the employee's injury to their employer, documenting the medical status and work capability of the injured employee, and specifying any work restrictions or necessary modifications based on the medical evaluation. Doctors and healthcare providers fill out the form after examining the injured employee, providing a detailed account of the employee’s current medical condition, work status, and any restrictions that should be considered by the employer. Carefully laid out, the DWC 73 form includes sections for general information about the injured employee, detailed work status information, specific activity restrictions if applicable, and instructions for follow-up treatment. It is designed to facilitate communication between medical providers, employees, employers, and insurance carriers, ensuring that all parties are informed about the employee’s health status and work capability. Understanding the specifics of how and when to file this form, as required by the Texas Administrative Code, is essential for compliance and to support the injured worker's recovery and return to work. For further assistance and clarification, the DWC offers free resources and guidance, advocating for the well-being and rights of injured workers within the state.
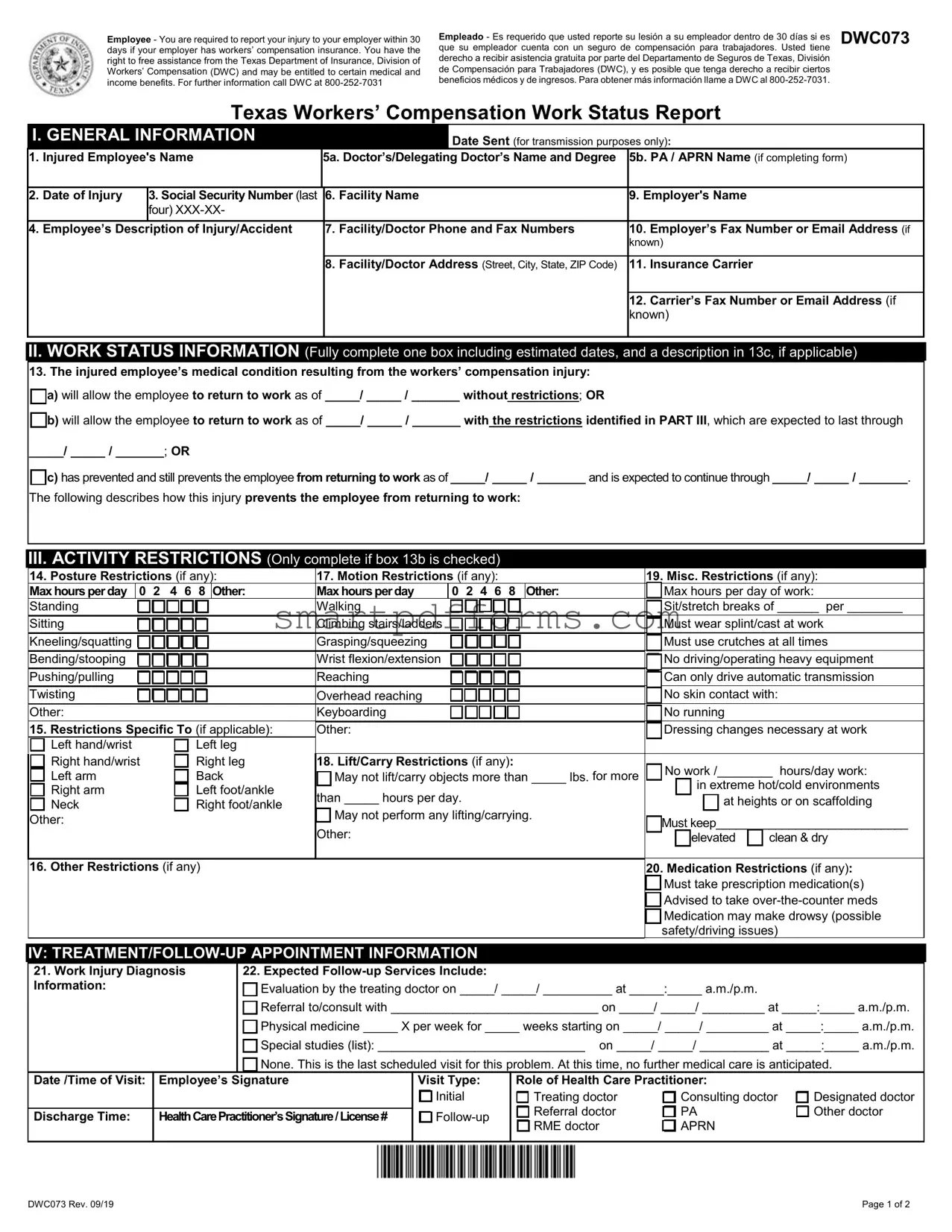
Preview - Dwc 73 Form
Employee - You are required to report your injury to your employer within 30 days if your employer has workers’ compensation insurance. You have the right to free assistance from the Texas Department of Insurance, Division of Workers’ Compensation (DWC) and may be entitled to certain medical and income benefits. For further information call DWC at
Empleado - Es requerido que usted reporte su lesión a su empleador dentro de 30 días si es |
DWC073 |
que su empleador cuenta con un seguro de compensación para trabajadores. Usted tiene |
|
derecho a recibir asistencia gratuita por parte del Departamento de Seguros de Texas, División de Compensación para Trabajadores (DWC), y es posible que tenga derecho a recibir ciertos beneficios médicos y de ingresos. Para obtener más información llame a DWC al
Texas Workers’ Compensation Work Status Report
I. GENERAL INFORMATION |
Date Sent (for transmission purposes only): |
|
1. |
Injured Employee's Name |
5a. Doctor’s/Delegating Doctor’s Name and Degree |
5b. PA / APRN Name (if completing form) |
||||
|
|
|
|
|
|
|
|
2. |
Date of Injury |
3. Social Security Number (last |
|
6. |
Facility Name |
9. Employer's Name |
|
|
|
four) |
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
Employee’s Description of Injury/Accident |
|
7. |
Facility/Doctor Phone and Fax Numbers |
10. |
Employer’s Fax Number or Email Address (if |
|
|
|
|
|
|
|
known) |
|
|
|
|
|
|
|
|
|
|
|
|
|
8. |
Facility/Doctor Address (Street, City, State, ZIP Code) |
11. |
Insurance Carrier |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. |
Carrier’s Fax Number or Email Address (if |
|
|
|
|
|
|
known) |
|
|
|
|
|
|
|
|
|
II.WORK STATUS INFORMATION (Fully complete one box including estimated dates, and a description in 13c, if applicable)
13.The injured employee’s medical condition resulting from the workers’ compensation injury:
a) will allow the employee to return to work as of _____/ _____ / _______ without restrictions; OR
b) will allow the employee to return to work as of _____/ _____ / _______ with the restrictions identified in PART III, which are expected to last through
_____/ _____ / _______; OR
c) has prevented and still prevents the employee from returning to work as of _____/ _____ / _______ and is expected to continue through _____/ _____ / _______.
The following describes how this injury prevents the employee from returning to work:
III.ACTIVITY RESTRICTIONS (Only complete if box 13b is checked)
|
14. Posture Restrictions (if any): |
17. Motion Restrictions (if any): |
|
|
|
|
19. Misc. Restrictions (if any): |
|||||||||||||||||||||||||||||
|
Max hours perday |
0 |
2 4 6 |
8 |
Other: |
Max hours perday |
|
0 2 4 6 8 |
|
|
Other: |
|
|
Max hours per day of work: |
||||||||||||||||||||||
|
Standing |
|
|
|
|
|
|
|
|
|
Walking |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sit/stretch breaks of ______ per ________ |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sitting |
|
|
|
|
|
|
|
|
|
Climbing stairs/ladders |
|
|
|
|
|
|
|
|
|
Must wear splint/cast at work |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Kneeling/squatting |
|
|
|
|
|
|
|
|
|
Grasping/squeezing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Must use crutches at all times |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Bending/stooping |
|
|
|
|
|
|
|
|
|
Wrist flexion/extension |
|
|
|
|
|
|
|
|
|
|
|
|
|
No driving/operating heavy equipment |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pushing/pulling |
|
|
|
|
|
|
|
|
|
Reaching |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Can only drive automatic transmission |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Twisting |
|
|
|
|
|
|
|
|
|
Overhead reaching |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No skin contact with: |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other: |
|
|
|
|
|
|
|
|
|
Keyboarding |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No running |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. Restrictions Specific To (if applicable): |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dressing changes necessary at work |
||||||||||||||||||
|
|
Left hand/wrist |
|
|
|
|
Left leg |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Right hand/wrist |
|
|
|
|
Right leg |
18. Lift/Carry Restrictions (if any): |
|
|
|
|
|
|
No work /________ |
hours/day work: |
||||||||||||||||||||
|
|
Left arm |
|
|
|
|
Back |
|
May not lift/carry objects more than _____ lbs. for more |
|
|
|||||||||||||||||||||||||
|
|
Right arm |
|
|
|
|
Left foot/ankle |
than _____ hours per day. |
|
|
|
|
|
|
|
|
in extreme hot/cold environments |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
at heights or on scaffolding |
||||||||||||||||||||||
|
|
Neck |
|
|
|
|
Right foot/ankle |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
May not perform any lifting/carrying. |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
Other: |
|
|
|
|
|
|
|
|
|
|
|
Must keep_____________________________ |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
elevated |
|
clean & dry |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16. Other Restrictions (if any) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. Medication Restrictions (if any): |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Must take prescription medication(s) |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Advised to take |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medication may make drowsy (possible |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
safety/driving issues) |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
IV: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
21. Work Injury Diagnosis |
|
|
|
22. Expected |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
Information: |
|
|
|
|
|
|
|
|
Evaluation by the treating doctor on _____/ _____/ __________ at _____:_____ a.m./p.m. |
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Referral to/consult with ______________________________ on _____/ _____/ _________ at _____:_____ a.m./p.m. |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Physical medicine _____ X per week for _____ weeks starting on _____/ _____/ _________ at _____:_____ a.m./p.m. |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Special studies (list): ______________________________ on _____/ _____/ __________ at _____:_____ a.m./p.m. |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
None. This is the last scheduled visit for this problem. At this time, no further medical care is anticipated. |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
Date /Time of Visit: |
Employee’s Signature |
|
|
Visit Type: |
|
Role of Health Care Practitioner: |
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Initial |
|
|
|
|
Treating doctor |
|
|
|
Consulting doctor |
Designated doctor |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Referral doctor |
|
|
|
PA |
|
Other doctor |
||
|
Discharge Time: |
HealthCarePractitioner’sSignature/License# |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
RME doctor |
|
|
|
APRN |
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DWC073 Rev. 09/19 |
Page 1 of 2 |
DWC073
Frequently Asked Questions
Work Status Report (DWC
Under what circumstances am I required to file DWC
Filing requirements for DWC
|
Type of Doctor |
|
|
When to File DWC |
|
|
|
Where to File |
|
|
Delivery Method |
|
|
Deadline |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treating Doctor |
• after the initial examination of the injured employee, |
|
• injured employee |
|
hand deliver; |
|
at the time of the |
|||||||
|
|
|
|
regardless of the employee’s work status |
|
|
|
|
|
electronic transmission, |
|
examination |
|||
|
Referral Doctor |
• when there is a change in the injured employee’s |
|
|
|
|
|
with agreement (fax, |
|
|
|
||||
|
|
|
|
work status |
|
|
|
|
|
email, or similar method) |
|
|
|
||
|
Delegated Physician |
• when there is a substantial change in the injured |
|
|
|
|
|
|
|
|
|
|
|||
|
Assistant (PA) |
|
employee’s activity restrictions |
|
|
|
|
|
|
|
|
|
|
||
|
or |
• on a schedule requested by the insurance carrier |
|
• insurance carrier |
|
electronic transmission |
|
within 2 working |
|||||||
|
|
as long as it is based on the injured employee’s |
|
|
|
|
|
|
|
|
days of the |
||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Delegated |
|
scheduled appointments with the doctor (not to |
|
|
|
|
|
|
|
|
examination |
|||
|
|
exceed one report every two weeks) |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
• employer |
electronic transmission |
|
|
|
||||||||
|
Advanced Practice |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
||||||||
|
Registered Nurse |
|
|
|
|
|
|
|
unless recipient has not |
|
|
|
|||
|
(APRN) |
|
|
|
|
|
|
|
provided a fax number or |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
email address; then by |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
personal delivery or mail |
|
|
|
||
|
|
|
• after receiving a set of functional job descriptions |
|
• injured employee |
|
hand deliver unless no |
|
within 7 days of |
||||||
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
||||||||||
|
|
|
|
from the employer or insurance carrier listing |
|
|
|
|
|
appointment is scheduled |
|
receiving job |
|||
|
|
|
|
modified duty positions, including the physical and |
|
|
|
|
|
before deadline; then |
|
description or |
|||
|
|
|
|
time requirements of the positions, that the |
|
|
|
|
|
electronic transmission |
|
RME opinion |
|||
|
|
|
|
employer has available for the injured employee to |
|
|
|
|
|
unless recipient has not |
|
|
|
||
|
|
|
|
work |
|
|
|
|
|
provided a fax number or |
|
|
|
||
|
|
|
• after receiving a DWC |
|
|
|
|
|
email address; then by |
|
|
|
|||
|
|
|
|
medical exam (RME) doctor that indicates the |
|
|
|
|
|
|
|
|
|||
|
|
|
|
injured employee can return to work with or without |
|
• insurance carrier |
|
electronic transmission |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
restrictions |
|
• employer |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
||||||||
|
Designated Doctor |
• after examination of an injured employee to |
|
• injured employee |
electronic transmission |
|
within 7 working |
||||||||
|
|
|
|
address any question relating to return to work |
|
• injured employee’s |
unless recipient has not |
|
days of the |
||||||
|
|
|
|
|
|
|
|
representative (if any) |
provided a fax number or |
|
examination |
||||
|
|
|
NOTE: The designated doctor must file a narrative |
|
|
|
|
email address; then by |
|
|
|
||||
|
|
|
report along with DWC |
|
|
|
|
other verifiable means |
|
|
|
||||
|
|
|
|
|
|
|
• insurance carrier |
|
electronic transmission |
|
|
|
|||
|
|
|
|
|
|
|
• treating doctor |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
• division |
|
fax to |
|
|
|
|||
|
|
|
|
|
|
|
|
||||||||
|
RME Doctor |
• after examination of an injured employee |
|
• injured employee |
electronic transmission |
|
within 7 days of |
||||||||
|
|
|
|
(subsequent to a Designated Doctor's |
|
• injured employee’s |
unless recipient has not |
|
the examination |
||||||
|
|
|
|
examination), if the RME doctor determines that the |
|
|
representative (if any) |
provided a fax number or |
|
|
|
||||
|
|
|
|
injured employee can return to work immediately |
|
|
|
|
email address; then by |
|
|
|
|||
|
|
|
|
with or without restrictions |
|
|
|
|
other verifiable means |
|
|
|
|||
|
|
|
|
|
|
|
• insurance carrier |
electronic transmission |
|
|
|
||||
|
|
|
|
|
|
|
• treating doctor |
|
|
|
|
|
|
||
Where can I find more information about DWC
For complete requirements regarding the filing of this report, see 28 Texas Administrative Code §§126.6, 127.10, and 129.5. These rules are available on the TDI website at http://www.tdi.texas.gov/wc/rules/index.html. If you have additional questions, call Comp Connection for Health Care Providers at
NOTE: With few exceptions, upon your request, you are entitled to be informed about the information DWC collects about you; to get and review the information (Government Code §§552.021 and 552.023); and to have DWC correct information that is incorrect (Government Code, §559.004). For more information, contact agencycounsel@tdi.texas.gov or you may refer to the Corrections Procedure section at www.tdi.texas.gov.
DWC073 Rev. 09/19 |
Page 2 of 2 |
Form Data
| Fact | Detail |
|---|---|
| Form Purpose | Texas Workers’ Compensation Work Status Report |
| Reporting Requirement | Employee must report injury within 30 days if employer has workers’ compensation insurance. |
| Assistance Available | Free assistance from the Texas Department of Insurance, Division of Workers’ Compensation. |
| Contact Information | For inquiries, call DWC at 800-252-7031. |
| Section I Content | General information including employee's name, date of injury, and employer’s details. |
| Section II Content | Work status information indicating the employee's capacity to return to work. |
| Activity Restrictions | Details on posture, motion, lifting, and medication restrictions, if any. |
| Section IV Content | Treatment/Follow-up appointment information with specifics on diagnosis and expected services. |
| Filing Requirements | Varies based on the type of doctor filing the report, with specific guidelines on when and where to file. |
| Governing Laws | 28 Texas Administrative Code §§126.6, 127.10, and 129.5. |
Instructions on Utilizing Dwc 73
After sustaining a work injury, it's crucial to communicate the injury specifics and work status clearly to ensure the injured employee can access the appropriate benefits and support. The Texas Workers’ Compensation Work Status Report, DWC 73 form, facilitates this process by allowing healthcare providers to outline the injured employee's ability to return to work, with or without restrictions, or the incapacity to work due to the injury. Prompt and accurate completion of this form is instrumental in managing the employee's recovery process and work status effectively.
- Enter the Date Sent at the top of the form, for transmission purposes only.
- Fill in the Injured Employee's Name under the GENERAL INFORMATION section.
- Provide the Date of Injury and the last four digits of the injured employee’s Social Security Number.
- Describe the injury or accident in the designated space.
- Include the Doctor’s/Delegating Doctor’s Name and Degree, and if applicable, the PA / APRN Name completing the form.
- Add the Facility Name, along with the Facility/Doctor Phone and Fax Numbers.
- Enter the Facility/Doctor Address (Street, City, State, ZIP Code).
- Include the Employer's Name, and if known, the Employer’s Fax Number or Email Address.
- Provide the name of the Insurance Carrier and, if known, the Carrier’s Fax Number or Email Address.
- In the WORK STATUS INFORMATION section, fully complete one box to indicate the injured employee's work status and include estimated dates and a description if applicable.
- If there are any activity restrictions, complete the ACTIVITY RESTRICTIONS section with appropriate details regarding posture, motion, and miscellaneous restrictions, including any specific limitations.
- Under the TREATMENT/FOLLOW-UP APPOINTMENT INFORMATION section, document the work injury diagnosis, expected follow-up services, and any scheduled appointments.
- Ensure the form is signed by the employee at the bottom, indicating acknowledgment of the reported status.
- Lastly, the health care practitioner must sign the form and provide their license number, specifying their role in the injured employee’s care.
Upon completion, the form should be filed according to the guidelines provided, ensuring it reaches the appropriate party—employer, insurance carrier, or both—within the specified deadlines to facilitate a smooth transition for the employee back into the workforce or ensure they receive suitable support during recovery.
Obtain Answers on Dwc 73
What is the DWC 73 form, and when is it required?
The DWC 73 form, also known as the Texas Workers' Compensation Work Status Report, is a crucial document in the workers' compensation process. It is used by doctors to report the work status of an employee who has suffered a work-related injury or illness. The form must be filed by the treating doctor after the initial examination of the injured employee, regardless of the employee's work status. If the employee sees a referral doctor or there is a substantial change in the employee's activity restrictions, the form must be updated and refiled. Additionally, if a functional job description is received, or after a required medical examination that indicates the injured employee can return to work with or without restrictions, the DWC 73 form should be completed and filed accordingly.
Where should the DWC 73 form be filed?
The DWC 73 form can be filed in several places, depending on who is completing the form. Typically, it should be filed with the injured employee and their insurance carrier. If the form is being completed by a delegated physician assistant, advanced practice registered nurse, or after receiving a functional job description or a sign-off from a required medical exam (RME) doctor, it may also need to be filed with the employer. The method of delivery can be through hand delivery, electronic transmission, personal delivery, or mail, depending on the recipient's availability of a fax number or email address.
What are the deadlines for filing the DWC 73 form?
The deadlines for filing the DWC 73 form vary based on the circumstances under which it is being filed. Generally, the form should be filed within two working days of the examination by a delegated physician assistant, and within seven working days for a designated doctor or an RME doctor's examination. It's important to adhere to these deadlines to ensure that the injured employee's work status is accurately and timely reported to all relevant parties.
How does the DWC 73 form impact an injured employee’s workers’ compensation benefits?
The DWC 73 form significantly impacts an injured employee's workers' compensation benefits by documenting the employee's ability to return to work and any restrictions that may affect their work capacity. This documentation is essential for determining the type and extent of benefits the injured employee may be entitled to receive, including medical and income benefits. Timely and accurate completion of this form can help ensure that employees receive the appropriate benefits and support during their recovery.
Are there any specific instructions for completing the activity restrictions section of the DWC 73 form?
Yes, the activity restrictions section of the DWC 73 form should be completed only if the box indicating that the injured employee can return to work with restrictions is checked. This section requires detailed information about any posture, motion, miscellaneous, lift/carry restrictions, and any medication restrictions that the injured employee has. These restrictions should be described clearly to inform the employer about the employee's limitations, helping to accommodate their return to work in a safe and suitable manner.
Where can I find more information and assistance regarding DWC Form-073?
More information regarding the DWC Form-073 can be found in the Texas Administrative Code §§126.6, 127.10, and 129.5, available on the TDI website. For additional questions or assistance, you can call Comp Connection for Health Care Providers at 1-800-372-7713 (or 512-804-4000 in the Austin area) and select option 3. This resource provides access to detailed guidelines and direct support for completing and filing the DWC 73 form correctly.
What happens if incorrect information is provided on the DWC 73 form?
If incorrect information is provided on the DWC 73 form, it may lead to delays or inaccuracies in the injured employee's workers' compensation benefits. It is crucial to ensure that all information on the form is accurate and complete. If an error is discovered, the Texas Department of Insurance, Division of Workers’ Compensation (DWC) allows individuals to request corrections. Contact agencycounsel@tdi.texas.gov or refer to the Corrections Procedure section on the DWC's website for more information on how to address and correct any inaccuracies on the form.
Common mistakes
When filing the DWC 73 form, also known as the Texas Workers' Compensation Work Status Report, accuracy is crucial to ensure that employees receive the benefits and support they're entitled to. However, individuals often encounter pitfalls that can complicate their claims. Here are 10 common mistakes to avoid:
- Not Reporting the Injury Within 30 Days: Failing to report your injury to your employer within the 30-day window can jeopardize your claim.
- Incomplete General Information: Skipping details in section I, such as the injured employee's name or the date of injury, can delay the processing of the report.
- Incorrect Social Security Number: Entering a wrong or incomplete Social Security number can lead to identification errors and subsequent delays.
- Vague Description of Injury/Accident: Not providing a clear and concise description of the injury or accident can make it difficult for the DWC to assess the case properly.
- Leaving Doctor's Information Blank: Not filling out the doctor’s or medical facility's information, including name, address, and contact details, can impede communication and processing.
- Unclear Work Status Information: Not fully completing one box in section II regarding the employee’s work status, including estimated dates for return, can lead to uncertainties about the employee's capabilities.
- Omitting Activity Restrictions: If section 13b is applicable, overlooking the completion of the activity restrictions can result in misunderstandings about the employee’s physical abilities and limitations at work.
- Miscategorizing Restrictions: Misidentifying or incorrectly listing restrictions, such as posture or motion restrictions, can lead to inappropriate work assignments or further injury.
- Forgetting Treatment/Follow-Up Appointment Information: Neglecting to provide upcoming treatment or follow-up appointments can hinder the DWC's ability to gauge the progress of recovery.
- Missing Signatures: Skipping the employee's or healthcare practitioner's signature can invalidate the report, as these are necessary for verification and processing.
To ensure that your DWC 73 form is correctly completed and submitted, careful attention to detail is key. By avoiding these common mistakes, employees can facilitate a smoother claim process, ensuring that they receive the appropriate medical and income benefits in a timely manner.
Documents used along the form
When managing workers' compensation claims in Texas, the DWC 73 form, or the Texas Workers' Compensation Work Status Report, plays a crucial role by providing an overview of an employee's work capabilities following an injury. However, to navigate the claims process effectively, several other forms and documents are commonly utilized in conjunction with DWC 73, each serving a specific purpose in the claim's administration and resolution.
- DWC 001: Employer's First Report of Injury or Illness – This document is filled out by the employer when an employee gets hurt at work. It details the circumstances of the injury and starts the claim process.
- DWC 041: Employee’s Claim for Compensation for a Work-Related Injury or Occupational Disease – Used by the employee to formally file a claim for workers' compensation benefits following an injury or diagnosis of a work-related illness.
- DWC 003: Employee's Wage Statement – This form provides information about the employee's earnings, which is essential for calculating compensation benefits accurately.
- TWCC-45: Request for Paid Leave – Employees fill out this form to request that their leave be paid while they are unable to work due to a work-related injury.
- DWC 069: Employee’s Request to Change Treating Doctors – If an employee wants to change their treating doctor, they must submit this form for approval to ensure continuity in their medical care and claims process.
- DWC 057: Request for Designated Doctor Examination – This form is used to request an examination by a designated doctor to resolve disputes about the employee's medical condition or impairment rating.
- DWC 025: Work Status Report – Similar to DWC 073 but used at different stages of treatment to continually update the employee's work status based on medical evaluations.
- DWC 064: Request for Social Security Number Release – Required when the employee's social security number is necessary for processing the claim and coordinating benefits.
- DWC 070: Benefit Dispute Agreement – This form is used when there is a dispute about the benefits, potentially leading to mediation or a contested case hearing to resolve the issue.
Together, these forms and documents facilitate a comprehensive approach to managing workers' compensation claims, ensuring that both the rights of the injured workers and the responsibilities of the employers are appropriately addressed. By utilizing these documents efficiently, stakeholders can navigate the complexities of the claims process, from injury reporting to the resolution of disputes and the provision of benefits.
Similar forms
The DWC 74 form, or the Texas Workers' Compensation Return-to-Work Guidelines, is closely related to the DWC 73 form. Both documents focus on the injured employee's ability to resume work after an injury. The DWC 74 specifically details possible modifications and restrictions to facilitate an injured employee's return, much like the DWC 73 form outlines specific activity restrictions and potential work status following an injury. Both forms are instrumental in communicating the injured worker's capabilities and restrictions between health care providers, employers, and insurance carriers.
DWC 69, the Texas Workers' Compensation Work Status Report, shares significant similarities with the DWC 73. Both serve as communication tools regarding an injured employee's work capabilities and limitations, ensuring that all parties involved in the workers' compensation claim process are informed about the employee's ability to work. However, while DWC 73 provides detailed information about specific restrictions and anticipated duration of such restrictions, DWC 69 often serves as the initial notification of an employee's injury status and their immediate work ability.
The DWC 48, Request for Designated Doctor Examination, although different in purpose from the DWC 73, still exhibits a level of similarity in the broader context of managing workers' compensation cases. This document is used to request a designated doctor to evaluate the extent of an injured employee's work-related injury or illness, potentially affecting the information reported on DWC 73 forms thereafter. Post-evaluation, the findings of a DWC 48 can dictate the conditions outlined in a DWC 73 form regarding an employee's work restrictions or readiness.
Form TWCC-45, Employee's Request for Dispute Resolution by Administrative Hearing, while primarily focused on disputes in the claims process, indirectly relates to the DWC 73 form. The outcomes of disputes, which might regard entitlements to certain medical or income benefits, or disagreements about work status determinations, can influence the contents of subsequent DWC 73 forms. Therefore, the resolution facilitated by a TWCC-45 filing has the potential to significantly alter the work status or restrictions reported on DWC 73, affecting an employee's return to work trajectory.
Dos and Don'ts
When filling out the DWC 73 form, an essential document for tracking an employee's work status following a work-related injury in Texas, it's crucial to understand the dos and don'ts. This guidance ensures the form is completed accurately and efficiently, providing all necessary information to the Texas Department of Insurance, Division of Workers' Compensation (DWC). Below is a list of practices to follow and to avoid:
- Do report your injury within 30 days to your employer if they have workers' compensation insurance.
- Do not delay seeking free assistance from the DWC if you have questions or need help filling out the form.
- Do ensure that all information, especially personal identifiers like the last four digits of your Social Security Number, is entered correctly.
- Do not leave sections incomplete; if a section does not apply, indicate with "N/A" for not applicable.
- Do provide a detailed employee’s description of the injury/accident to ensure clarity on the event and its impact.
- Do not guess on dates and specifics regarding the injury or work status; confirm all details for accuracy before submitting.
- Do clearly specify any restrictions in the activity restrictions section if the employee cannot return to work without limitations.
- Do not sign the document without reviewing all filled-out information for accuracy and completeness.
- Do use the correct delivery method and meet the filing deadline as specified under different circumstances in the form instructions.
Following these guidelines will help ensure that the DWC 73 form is filled out correctly and submitted appropriately, facilitating a smoother process for workers' compensation benefits.
Misconceptions
Understanding the complexities of workers’ compensation forms can be challenging for both employees and employers. The DWC 73 form, also known as the Texas Workers’ Compensation Work Status Report, is a crucial document in the process. Nevertheless, several misconceptions exist regarding its usage and significance. Let’s clarify some of these misunderstandings.
- Misconception 1: The DWC 73 form is only for the employer’s benefit.
Contrary to what some might believe, the DWC 73 form serves both the employee and the employer. It provides a formal way to communicate the injured worker's medical status and work abilities to the employer, ensuring that work assignments match the employee’s medical restrictions, if any. - Misconception 2: The form is optional if the injury seems minor.
Regardless of the injury's apparent severity, completing the DWC 73 is essential. It officially documents the injury and the medical professional’s advice, protecting the rights and interests of both the employee and the employer. - Misconception 3: Any health care provider can complete the form.
While it might seem efficient for any health provider to fill this out, the DWC 73 form requires completion by specific professionals involved in the employee's care following a work-related injury. This includes the treating doctor, referral doctors, delegated physician assistants, or advanced practice registered nurses, under certain conditions. - Misconception 4: The DWC 73 is just a one-time report.
This report may need to be updated and resubmitted if there’s a substantial change in the employee’s condition, work status, or if the medical professional recommends different restrictions. It’s not just a one-off; it's part of ongoing communication during the employee's recovery process. - Misconception 5: Employees do not need to understand what’s on the DWC 73.
It’s vital for employees to understand the contents of the DWC 73 form since it outlines their current work abilities and any restrictions. Being aware and in agreement with what's documented can help prevent misunderstandings and ensure that they do not undertake tasks that could hinder their recovery.
Clearing up these misconceptions is key to ensuring that the DWC 73 form is used effectively, fostering a smoother recovery and return-to-work process for injured employees. Remember, open communication and a clear understanding of this document can significantly impact the successful management of work-related injuries.
Key takeaways
Understanding the intricacies of the DWC 73 form, officially known as the Texas Workers’ Compensation Work Status Report, is crucial for both employers and employees navigating the workers' compensation process in Texas. Here are four key takeaways to ensure accurate filling out and use of this important document.
- Timely Reporting is Crucial: Employees must report their injury to their employer within 30 days if the employer has workers' compensation insurance. This initial step is vital for preserving the right to potential medical and income benefits. The DWC 73 form plays a critical role in this process by documenting the injury and its impact on the employee's work status.
- Detailed Medical Condition Reporting: The form requires a comprehensive account of the injured employee's medical condition and how it affects their capability to work. This includes whether the employee can return to work with or without restrictions, or if they are unable to return to work due to their condition. Ensuring that this section is filled out with precision is key to communicating the needed accommodations or restrictions to the employer and insurance carrier.
- Activity Restrictions Must Be Clearly Defined: If the employee has restrictions, Section III (Activity Restrictions) of the form needs to be completed detailing posture, motion, and miscellaneous restrictions among others. This includes specifying maximum hours per day for certain activities, and if any medical aids (like splints or crutches) are necessary at work. Accurate completion helps in formulating a suitable work plan that considers the employee’s health restrictions.
- Follow-Up Treatment and Appointments: Information about the diagnosis, expected follow-up services, and details of any scheduled appointments for evaluation or treatment must be provided in Section IV. This section ensures that there is a clear plan for the employee's recovery and return to work pathway, including any anticipated medical care or assessments.
Both employees and employers benefit from an accurately completed DWC 73 form. For employees, it is a key document that supports their claim for workers’ compensation benefits including necessary medical care and possible income benefits. For employers and insurance carriers, it provides essential information to accommodate the injured employee’s return to work in a safe and appropriate manner. Familiarity with the DWC 73 form and its requirements can significantly streamline the workers' compensation process.
Popular PDF Forms
Hvcc Appraisal - An official confirmation from the lender that the valuation process and final appraisal report adhered strictly to the conditions and standards prescribed by HVCC.
Cn22 Form - The ability to indicate an office of origin and date of posting documents the shipment's starting point, aiding in tracking and provenance verification.
Topgrading Career History Form - Assurance of a thorough review of statements made on the form as part of a comprehensive evaluation process aimed at fair and informed hiring decisions.