Blank Employee Call Off Sheet PDF Template
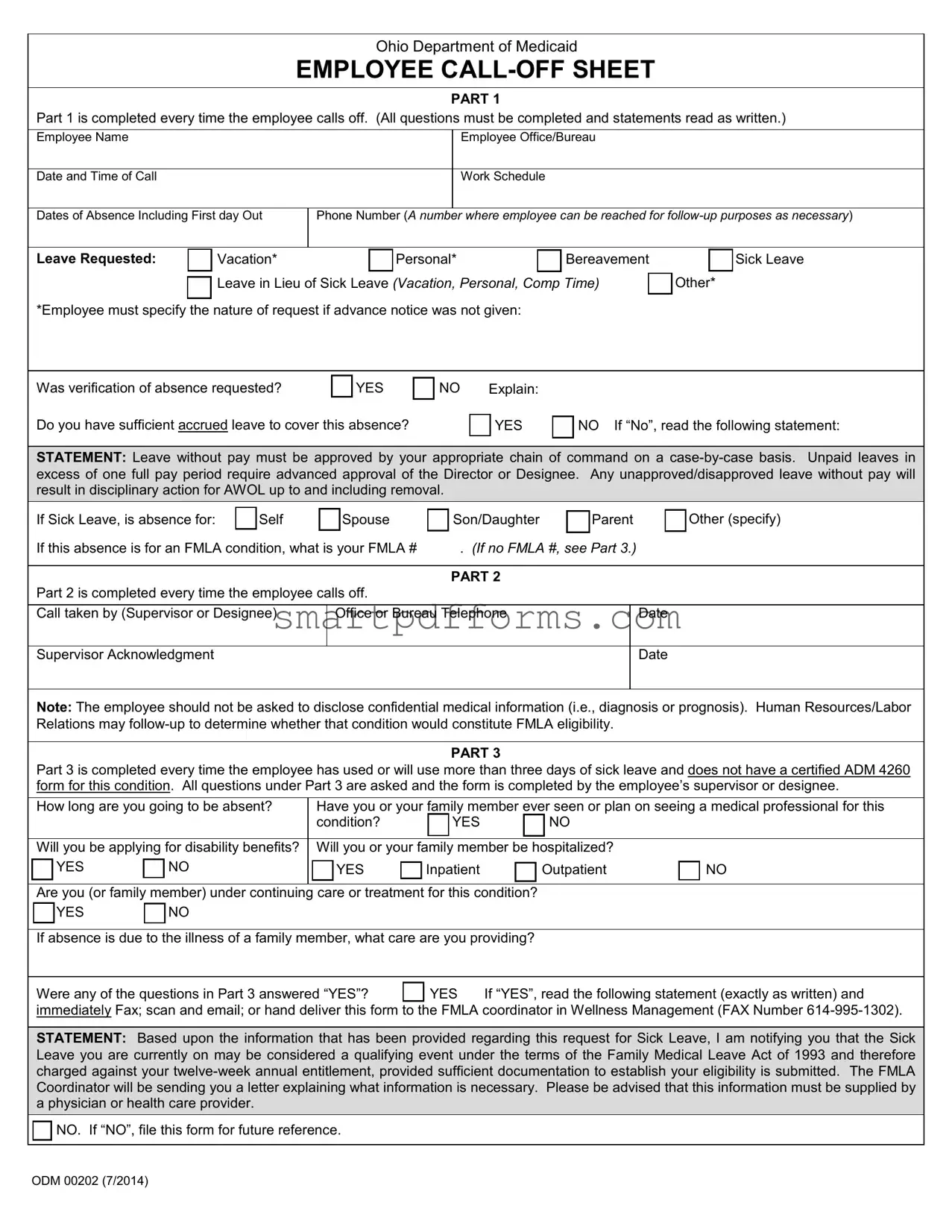
In the workplace, managing absences effectively is crucial to maintaining productivity and ensuring fair treatment of employees. The Ohio Department of Medicaid's Employee Call Off Sheet form serves as a structured approach for employees to report absences. Through a comprehensive three-part process, the form captures essential information each time an employee needs to call off from work, facilitating clear communication between employees and management. Part 1 requires employees to provide detailed information regarding the nature of their absence, including the type of leave requested and verification of accrued leave adequate to cover the absence. Importantly, it sets out the conditions under which unpaid leave may be considered and the potential consequences for unapproved leaves. Part 2 is geared toward supervisor acknowledgment, emphasizing the importance of maintaining privacy regarding medical information while assessing the situation's compatibility with the Family and Medical Leave Act (FMLA) provisions. Part 3 delves deeper in cases where sick leave extends beyond three days without a certified form, probing into the necessity for medical care and potential FMLA eligibility. This thorough documentation process underscores the balance between employee rights and organizational policies, aiming to streamline the absence reporting mechanism while aligning with legal frameworks such as FMLA.
Preview - Employee Call Off Sheet Form
Ohio Department of Medicaid
EMPLOYEE
PART 1
Part 1 is completed every time the employee calls off. (All questions must be completed and statements read as written.)
Employee Name
Employee Office/Bureau
Date and Time of Call
Work Schedule
Dates of Absence Including First day Out
Phone Number (A number where employee can be reached for
Leave Requested: |
|
Vacation* |
|
Personal* |
|
Bereavement |

 Leave in Lieu of Sick Leave (Vacation, Personal, Comp Time)
Leave in Lieu of Sick Leave (Vacation, Personal, Comp Time)
*Employee must specify the nature of request if advance notice was not given:

 Sick Leave Other*
Sick Leave Other*
Was verification of absence requested? |
YES |
Do you have sufficient accrued leave to cover this absence?
NO Explain:
YES
NO If “No”, read the following statement:
STATEMENT: Leave without pay must be approved by your appropriate chain of command on a
If Sick Leave, is absence for:
Self
Spouse
Son/Daughter |
|
Parent |
|
Other (specify) |
If this absence is for an FMLA condition, what is your FMLA # |
. (If no FMLA #, see Part 3.) |
PART 2
Part 2 is completed every time the employee calls off.
Call taken by (Supervisor or Designee)
Office or Bureau Telephone
Date
Supervisor Acknowledgment
Date
Note: The employee should not be asked to disclose confidential medical information (i.e., diagnosis or prognosis). Human Resources/Labor Relations may
PART 3
Part 3 is completed every time the employee has used or will use more than three days of sick leave and does not have a certified ADM 4260 form for this condition. All questions under Part 3 are asked and the form is completed by the employee’s supervisor or designee.
|
How long are you going to be absent? |
|
Have you or your family member ever seen or plan on seeing a medical professional for this |
||||||||||||||
|
|
|
|
|
|
condition? |
|
|
|
YES |
|
|
NO |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Will you be applying for disability benefits? |
|
Will you or your family member be hospitalized? |
|
|
||||||||||||
|
|
YES |
|
NO |
|
|
YES |
|
Inpatient |
|
|
Outpatient |
|
NO |
|||
|
|
|
|
|
|
|
|
|
|||||||||
Are you (or family member) under continuing care or treatment for this condition?
YES |
NO |
If absence is due to the illness of a family member, what care are you providing?
Were any of the questions in Part 3 answered “YES”? |
|
YES |
If “YES”, read the following statement (exactly as written) and |
|
immediately Fax; scan and email; or hand deliver this form to the FMLA coordinator in Wellness Management (FAX Number |
||||
STATEMENT: Based upon the information that has been provided regarding this request for Sick Leave, I am notifying you that the Sick Leave you are currently on may be considered a qualifying event under the terms of the Family Medical Leave Act of 1993 and therefore charged against your

 NO. If “NO”, file this form for future reference.
NO. If “NO”, file this form for future reference.
ODM 00202 (7/2014)
Form Data
| Fact Name | Description |
|---|---|
| Form Identification | The form is known as the Employee Call-Off Sheet, designated by the Ohio Department of Medicaid with the form number ODM 00202 (7/2014). |
| Primary Purpose | Part 1 is used to document each instance an employee calls off from work, requiring detailed information including the reason for absence and leave requested. |
| Required Information | Employees must provide their name, office/bureau, date and time of the call, work schedule, dates of absence, a contact number, and the type of leave requested. |
| Verification of Absence | The form asks whether verification of absence was requested and if the employee has sufficient accrued leave to cover their absence. |
| Statement on Leave Without Pay | Employees are alerted that leave without pay requires approval and may lead to disciplinary action if unapproved, especially if it exceeds one full pay period. |
| Provisions for Family Medical Leave Act (FMLA) | Part 3 guides on the steps to follow if the sick leave might be a qualifying event under FMLA, including the potential need to submit documentation from a health care provider. |
| Governing Law | This form is governed under the laws of the state of Ohio, with specific reference to ensuring compliance with the Family Medical Leave Act of 1993. |
Instructions on Utilizing Employee Call Off Sheet
Filling out the Employee Call Off Sheet form is an essential task when you need to report an absence from work. It ensures clear communication between employees and their supervisors regarding the leave requested, be it for personal reasons, sickness, or another approved absence type. This form is particularly used by employees of the Ohio Department of Medicaid and it captures the necessary details to process the absence properly. Below are the steps to fill out the form effectively.
- Employee Name: Start by writing your full name as it appears in your employment records.
- Employee Office/Bureau: Input the specific office or bureau where you are assigned.
- Date and Time of Call: Note the date and time when you made the call to inform your employer of the absence.
- Work Schedule: Provide the normal work hours that you were scheduled to work on the day(s) you are calling off.
- Dates of Absence Including First Day Out: Clearly state the starting date of your absence and how many days you anticipate being out.
- Phone Number: Write down a contact number where you can be reached if any follow-up is necessary regarding your absence.
- Leave Requested: Specify the type of leave you are requesting (e.g., vacation, personal, bereavement, sick leave). If the leave was not requested in advance, detail the nature of the request.
- Was verification of absence requested? Indicate with a YES or NO whether you were asked to provide verification for your absence.
- Do you have sufficient accrued leave to cover this absence? Answer YES or NO. If "No," read and acknowledge the subsequent statement regarding unpaid leave.
- If Sick Leave: If you're taking sick leave, specify whom the leave is for (e.g., self, spouse, son/daughter, parent, other).
- If this absence is for an FMLA condition: Provide your FMLA number. If you do not have an FMLA number, note that and see Part 3 of the form.
- Call taken by: Enter the name of your supervisor or their designee who received your call-off.
- Office or Bureau Telephone: Write the telephone number of the office or bureau where your supervisor works.
- Date: Note the date when your call-off was acknowledged by a supervisor.
- Supervisor Acknowledgment Date: The supervisor acknowledges the call-off by noting the date.
After completing the form, your supervisor will review the information and may follow up with additional steps if your sick leave extends beyond three days or if your situation qualifies for Family Medical Leave Act (FMLA) considerations. Ensure all parts of the form are filled in accurately to avoid delays in processing your absence. Remember, your supervisor or HR department can assist with any uncertainties when completing the form.
Obtain Answers on Employee Call Off Sheet
What is the purpose of completing the Employee Call Off Sheet form each time an employee calls off work?
The Employee Call Off Sheet form serves multiple important purposes. Initially, it provides a structured method for employees to report their absence from work, ensuring all relevant information is neatly documented. This includes details like the reason for the absence, the duration, and whether the leave is paid or unpaid. By doing so, it aids in maintaining a clear record for payroll and leave management purposes. Moreover, the form assists in determining eligibility for certain types of leave, such as the Family Medical Leave Act (FMLA), by capturing necessary details that could qualify an absence under this law. Thus, it not only ensures compliance with organizational policies but also with relevant laws and regulations.
How should an employee fill out the form if they do not have a Family Medical Leave Act (FMLA) number but believe their absence might qualify?
If an employee lacks an FMLA number but suspects their absence might qualify under FMLA, they should still complete the form as thoroughly as possible. Specifically, in the section where the FMLA number is requested, the employee should indicate the absence of a number and see Part 3 for further instructions. They are also advised to immediately contact the FMLA coordinator as indicated in Part 3, providing all requested details about their condition. The FMLA coordinator will then guide them through the process of obtaining an FMLA number, if applicable, and inform them of the documentation needed to establish eligibility for FMLA leave.
What happens if an employee doesn't have enough accrued leave to cover their absence?
If an employee doesn't have sufficient accrued leave to cover their absence, the form instructs them to read a specific statement outlining the next steps. Leave without pay may be granted, but it requires approval from the employee’s chain of command on a case-by-case basis. If the unpaid leave exceeds one full pay period, advanced approval from the Director or their designee is mandatory. It's crucial for employees to understand that any unapproved or disapproved leave without pay might lead to disciplinary action for being absent without leave (AWOL), potentially including termination. Employees in this situation are encouraged to communicate with their supervisors or human resources department to explore their options.
Is confidential medical information required when completing the form?
No, the Employee Call Off Sheet form explicitly states that employees should not be asked to disclose confidential medical information, such as a diagnosis or prognosis. This provision safeguards employee privacy and complies with legal standards regarding medical confidentiality. However, for absences that may qualify for FMLA leave or other similar provisions, Human Resources or Labor Relations may follow up to determine the nature of the condition—whether it constitutes FMLA eligibility—without requiring specific medical details. Employees will only need to provide documentation from a physician or healthcare provider if their leave is potentially covered under FMLA, as directed by the FMLA coordinator.
Common mistakes
When filling out the Employee Call Off Sheet, which is crucial for accurate record-keeping and compliance with organizational as well as legal standards, individuals frequently encounter several pitfalls. Recognizing and avoiding these mistakes can ensure the process aligns with the requirements, ultimately facilitating a smooth administrative process.
- Not completing every question in Part 1 every time they call off. It's imperative to provide all requested details to ensure proper documentation and follow-up if necessary.
- Omitting the nature of the leave request when no advance notice was given. For example, failing to specify whether the leave is for sickness or another reason when advance notice hasn't been provided.
- Forgetting to state whether they have sufficient accrued leave to cover the absence. This oversight can lead to unauthorized leave and potential disciplinary action.
- Incorrectly answering or skipping the question about whether verification of absence was requested. This can affect the legitimacy of the leave request and subsequent follow-ups.
- Neglecting to complete Part 2 of the form, which is required with every call-off. This part is crucial for supervisor acknowledgment and proper documentation.
- Failing to properly identify the type of leave requested, such as vacation, personal, or sick leave. This can lead to incorrect recording of leave types and affect leave balances.
- Overlooking the need to specify the relationship of the person for whom the employee is taking sick leave (e.g., self, spouse, son/daughter, etc.). This detail is essential for FMLA considerations and other leave policies.
- Not accurately indicating FMLA status or number, especially when the absence is for an FMLA-qualified condition. This error can complicate FMLA tracking and compliance.
- Omitting details in Part 3 regarding the duration of the absence, medical professional consultations, and care provisions for family members. These details are crucial for determining FMLA eligibility and other leave entitlements.
These common mistakes underline the importance of attention to detail and full compliance with the form's instructions. Employees should be encouraged to meticulously review the form before submission to avoid errors that could impact their leave status and the organization's record-keeping.
Documents used along the form
When managing employee absences, it's crucial to have a systematic approach to document and track these occurrences. The Employee Call Off Sheet is a fundamental component of this system, particularly within the framework of the Ohio Department of Medicaid. To complement this form and ensure a comprehensive absence management system, several other documents are typically utilized. Understanding each document's purpose can enhance both compliance and efficiency in managing workplace absences.
- Absence Request Form: Employees fill this out to formally request time off for vacation, personal leave, or any other non-sick related absence. It's a proactive document, usually submitted well in advance of the requested time off.
- Medical Certification Form: For absences due to illness, this form, completed by a healthcare provider, verifies the need for medical leave and clarifies the employee's ability to return to work.
- Return to Work Form: After a medical-related absence, employees present this document, often completed by their healthcare provider, indicating they are cleared to resume work responsibilities.
- Family and Medical Leave Act (FMLA) Application: This is required when an employee needs an extended leave for reasons covered under FMLA. It involves detailed information about the nature of the leave request and eligibility documentation.
- Attendance Record: This log tracks an employee’s presence, tardiness, and absences over a period. It's essential for evaluating patterns and compliance with company attendance policies.
- Leave Balance Report: Provides current information on the amount of leave (sick, personal, vacation) an employee has left, helping both the employee and management plan for absences better.
- Employee Warning Notice: Used to document and communicate disciplinary actions related to unauthorized or excessive absences, this notice serves as a formal record of an employee's attendance issue.
- Time Off Request Email Template: A pre-designed format for employees to request time off via email, ensuring all necessary information is provided and requests are standardized.
- Emergency Contact Form: Although not directly related to absence management, this form is crucial for maintaining current contact information for each employee, which can become relevant in the event of an unexpected absence.
These documents form a network of procedural support for managing employee absences, ensuring both employer and employee obligations are met with clarity and consistency. By integrating the Employee Call Off Sheet with these additional forms and documents, employers can effectively manage absences while supporting a productive and compliant work environment. Familiarity with each document ensures that absences, whether planned or unexpected, are handled efficiently and with the necessary attention to detail and record-keeping requirements.
Similar forms
Time-Off Request Form: Similar to the Employee Call Off Sheet, Time-Off Request Forms are used by employees to request leave from work. Both forms capture essential details such as the employee's name, dates of absence, and the type of leave requested. However, while the Time-Off Request Form is usually submitted in advance of the absence, the Employee Call Off Sheet is filled out when an absence is unexpected or last-minute.
Absence Notification Email Template: This document serves a similar purpose to the Employee Call Off Sheet by notifying the relevant supervisors about an employee's absence. Both contain key information such as the date and reason for absence. The main difference lies in the medium – one is a standardized form, and the other is a more flexible email format.
Leave of Absence Form: Used for requesting extended time off, this form shares similarities with the Employee Call Off Sheet, especially for longer absences. Both forms require details about the leave type (e.g., sick leave, personal leave) and the expected duration of the absence. The key distinction is that Leave of Absence Forms typically undergo a more rigorous approval process due to the extended time off work.
Family and Medical Leave Act (FMLA) Request Form: This form is used when an employee needs to take leave for reasons specified under the FMLA, which can include personal or family illness. The Employee Call Off Sheet covers some overlapping areas, such as inquiring if the absence is for an FMLA-qualifying event. Both forms require verification and processing by Human Resources, aiming to determine the eligibility for the requested leave.
Sick Leave Certification Form: Similar to the Employee Call Off Sheet, particularly Part 3, the Sick Leave Certification Form requests detailed information about the illness or condition leading to an employee's absence. It usually requires a healthcare provider's certification, emphasizing the serious nature of the leave request. Both forms contribute to the administrative process of verifying the need for and legitimacy of sick leave.
Return to Work Form: Often completed after an absence, this form complements the Employee Call Off Sheet by confirming that an employee is medically fit to resume work, particularly after a sick leave. While the Call Off Sheet documents the beginning of an absence, the Return to Work Form bookends the absence, ensuring a smooth transition back to the workplace.
Doctor’s Note: This document might not be a form per se but serves a similar function to parts of the Employee Call Off Sheet, especially when an employee is instructed to follow up with documentation from a healthcare provider. Both convey health-related reasons for an absence and often require validation from a medical professional to justify time off work.
Emergency Contact Form: Though not directly related to reporting absences, this form contains personal information that might be necessary in case an employee's health situation during work leads to an emergency. Similar to the Employee Call Off Sheet, it deals with scenarios where personal and health information may inform or affect workplace attendance and procedures.
Dos and Don'ts
When you're filling out the Employee Call Off Sheet form, it's important to follow a few dos and don'ts to ensure the process is completed accurately and efficiently. Here's a guide to help you through:
Do:- Complete all sections: Ensure every question in Part 1 is filled out every time an employee calls off. This includes providing detailed information about the absence, such as the nature of the leave requested and whether advance notice was given.
- Be precise with dates: Clearly indicate the dates of absence, including the first day out. Accuracy here is crucial for record-keeping and auditing purposes.
- Provide a reachable phone number: List a contact number where the employee can be reached for any follow-up. This is necessary for any clarifications or additional information that may be required.
- Specify the type of leave: Clearly identify the type of leave being requested (e.g., Sick Leave, Vacation, Personal, etc.). If sick leave is chosen, specify whom it's for (self, spouse, etc.).
- Follow up with Human Resources/Labor Relations if needed: This is important, especially if the absence could qualify for FMLA. HR can help with the FMLA certification process.
- Leave sections incomplete: Skipping questions or sections can lead to the form being returned for completion, delaying the process.
- Disclose confidential medical information: While the form requires some information about the nature of the absence, specific diagnoses or medical conditions should not be included. This information is private and protected.
- Forget to indicate the FMLA number if applicable: If the absence is related to an FMLA-covered condition and you have an FMLA number, make sure to include this on the form.
- Ignore the instructions for leave without pay: If you don't have sufficient accrued leave to cover the absence, read and understand the implications as outlined in the form. Failure to comply with these instructions can lead to disciplinary action.
Correctly filling out the Employee Call Off Sheet not only helps in efficient record-keeping but also ensures that employees' rights and entitlements are preserved. It's vital for both the employee's and the organization's benefit to adhere to these guidelines.
Misconceptions
- One common misconception is that the Employee Call Off Sheet is only used for reporting sick leave. However, this form also covers other types of leave such as vacation, personal, bereavement, and leave in lieu of sick leave. Employees are required to specify the nature of their absence, whether it's for illness or another reason, especially if advance notice was not given. This broadens the scope of the form beyond just health-related absences.
- Many people believe that the Employee Call Off Sheet invades privacy by requiring detailed medical information. The truth is, the form explicitly states that employees should not be asked to disclose confidential medical information, like a diagnosis or prognosis. Follow-up regarding eligibility for certain types of leave, such as the Family Medical Leave Act (FMLA), will be handled by Human Resources/Labor Relations, ensuring confidentiality and compliance with privacy regulations.
- Another misconception is that filling out the Employee Call Off Sheet guarantees the approval of requested leave. The form does include a section where employees must state whether they have accrued enough leave to cover their absence, and it warns that leave without pay must be approved on a case-by-case basis by the appropriate chain of command. Unapproved or disapproved leave without pay could result in disciplinary action, indicating that not all leave requests may be granted as expected.
- Finally, it’s mistakenly believed that the Employee Call Off Sheet is only relevant at the time of the call-off. In reality, Part 3 of the form becomes crucial if the employee uses more than three days of sick leave and doesn’t have a certified ADM 4260 form for the condition. This part of the form, filled out by the employee's supervisor or designee, helps identify if the sick leave could qualify as an FMLA event, thereby potentially affecting the employee's annual FMLA entitlement. This indicates the form also plays a role in managing longer-term absences.
Key takeaways
The process of filling out and utilizing the Employee Call Off Sheet, as outlined by the Ohio Department of Medicaid, is crucial for both employees and employers to understand. It serves as a formal record of an employee's request for time off and plays a vital role in the management of leave within an organization. Here are five key takeaways from this document:
- Comprehensive information is required: Every time an employee needs to call off, they must fill out Part 1 of the form in its entirety. This includes providing their name, office or bureau, date and time of the call, work schedule, dates of absence, a reachable phone number, and the type of leave requested. Failure to complete all questions and statements as required may affect the processing of the leave request.
- Clarification on the type of leave requested: The employee must specify the nature of their leave request, particularly if advance notice was not given. This includes whether the leave is for vacation, personal reasons, bereavement, or in lieu of sick leave. For sick leave, further details such as whether the absence is for the employee themselves or a family member, and if it relates to an FMLA condition, must be provided.
- Approval and verification requirements: The form explicitly states that leave without pay requires approval from the appropriate chain of command and that unwarranted unpaid leaves may lead to disciplinary action. Additionally, supervisors may request verification of absence to ensure compliance with organizational policies, though it's explicit that medical details should remain confidential.
- The role of supervisors and HR: After an employee calls off, a supervisor or designee is responsible for completing Part 2 of the form, which acknowledges the call-off. Human Resources or Labor Relations may follow up to ascertain FMLA eligibility without requiring the disclosure of confidential medical information.
- Implications for extended sick leave: If an employee indicates that they or their family member will see a medical professional or be hospitalized, this may trigger eligibility for FMLA leave. Part 3 of the form is geared towards identifying conditions that qualify for extended sick leave under FMLA, with a specific statement to be read to the employee about potential FMLA qualification if certain conditions are met.
Properly completing and managing the Employee Call Off Sheet is essential for ensuring that leave is administered fairly and consistently, aligning with legal requirements and organizational policies. It acts as a safeguard for both the employee's rights and the employer's operational needs.
Popular PDF Forms
How to Write a Landscaping Contract - Outlining detailed service tasks, such as the removal of weeds and grass from cracks, highlights Goodman’s attention to detail in maintaining property aesthetics.
Non Cash Charitable Contributions - Allows taxpayers to substantiate their claims for tax deductions with precise details about their charitable donations of property.
Right to Lien Notice - This letter acts as a warning to the property owner, stating the amount owed for services rendered on a residential project and the intent to secure payment through legal means.