Blank H1836 A PDF Template
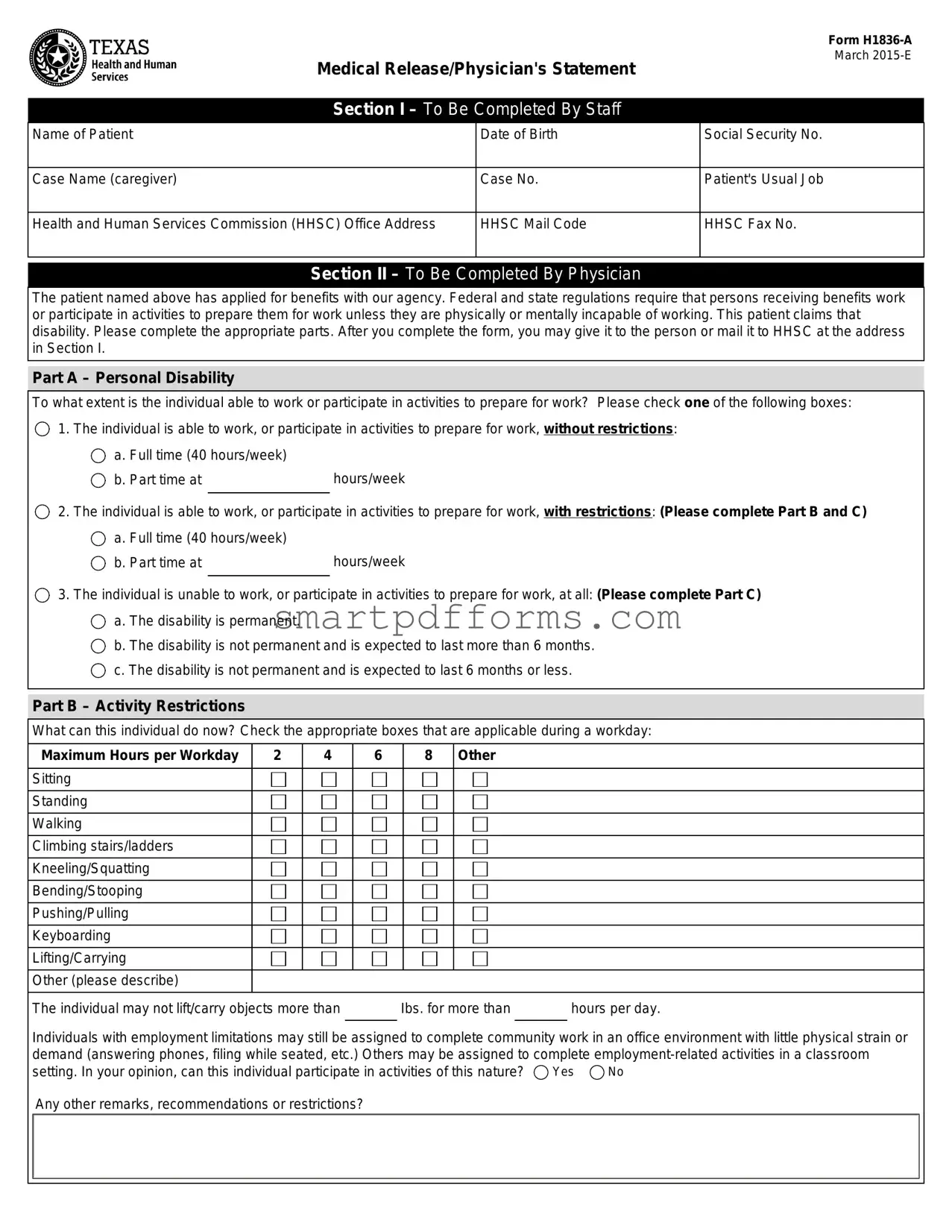
Engaging with the H1836-A form, commonly known as the Medical Release/Physician's Statement, unveils a critical procedural element for individuals applying for benefits through various health and social services programs. Issued in March 2015, this document serves as a linchpin for confirming an applicant's claims of physical or mental incapacity to work, as mandated by federal and state regulations. The form is meticulously divided into sections, each designated for completion by specific parties, starting with information filled out by staff regarding the patient, including biographical details and case information. The crux of the form lies in the second section, which requires thorough completion by a certified physician. This part delves into the patient's current ability to work or participate in work-preparation activities, further segmented into assessments of personal disability, activity restrictions, and diagnoses, thereby painting a comprehensive picture of the individual's physical and work-related capabilities. Additionally, it touches upon potential participation in less physically demanding tasks, underscoring the form's role in determining suitability for various types of employment or exemptions. The final section shifts focus to the patient (or their representative), emphasizing the voluntary nature of authorizing medical information release for the sole purpose of substantiating claims to the Health and Human Services Commission (HHSC) and potentially the Texas Workforce Commission. This authorization highlights privacy concerns and the safeguarding of personal health information, referencing the expiration of consent and the process to retract permission, all of which demonstrate the intricate balance between applicant rights and program eligibility requirements.
Preview - H1836 A Form
Medical Release/Physician's Statement
Form
March
Section I – To Be Completed By Staff
Name of Patient |
Date of Birth |
Social Security No. |
|
|
|
Case Name (caregiver) |
Case No. |
Patient's Usual Job |
|
|
|
Health and Human Services Commission (HHSC) Office Address |
HHSC Mail Code |
HHSC Fax No. |
|
|
|
Section II – To Be Completed By Physician
The patient named above has applied for benefits with our agency. Federal and state regulations require that persons receiving benefits work or participate in activities to prepare them for work unless they are physically or mentally incapable of working. This patient claims that disability. Please complete the appropriate parts. After you complete the form, you may give it to the person or mail it to HHSC at the address in Section I.
Part A – Personal Disability
To what extent is the individual able to work or participate in activities to prepare for work? Please check one of the following boxes:
1. The individual is able to work, or participate in activities to prepare for work, without restrictions:
a. Full time (40 hours/week) |
|
b. Part time at |
hours/week |
2. The individual is able to work, or participate in activities to prepare for work, with restrictions: (Please complete Part B and C)
a. Full time (40 hours/week) |
|
b. Part time at |
hours/week |
3. The individual is unable to work, or participate in activities to prepare for work, at all: (Please complete Part C)
a. The disability is permanent.
b. The disability is not permanent and is expected to last more than 6 months.
c. The disability is not permanent and is expected to last 6 months or less.
Part B – Activity Restrictions
What can this individual do now? Check the appropriate boxes that are applicable during a workday:
Maximum Hours per Workday |
2 |
4 |
6 |
8 Other |
Sitting
Standing
Walking
Climbing stairs/ladders
Kneeling/Squatting
Bending/Stooping
Pushing/Pulling
Keyboarding
Lifting/Carrying
Other (please describe)
The individual may not lift/carry objects more than Ibs. for more than hours per day.
Individuals with employment limitations may still be assigned to complete community work in an office environment with little physical strain or demand (answering phones, filing while seated, etc.) Others may be assigned to complete
setting. In your opinion, can this individual participate in activities of this nature? |
Yes |
No |
Any other remarks, recommendations or restrictions?
Form
|
|
|
|
Page 2 / |
|
|
|
|
|
Part C – Diagnosis |
|
|
|
|
Primary Disabling Diagnosis |
|
|
Secondary Disabling Diagnosis |
|
|
|
|
|
|
Comments |
|
|
|
|
|
|
|
|
|
Name of Physician (please type or print) |
Signature – Physician |
Date |
||
|
|
|
|
|
Physicians License No. |
Office Address (Street or P.O. Box, City, State and ZIP) |
Area Code and Phone No. |
||
|
|
|
|
|
Section III – To Be Completed By Patient or Patient's Personal Representative
Authorization to Release Medical Information
Patient's Name:
HHSC is requesting verification of the medical condition that prevents you from participating in the employment services program. When you sign this authorization, you are giving HHSC permission to contact your doctors, medical facilities or other health care providers to request copies of your health information as indicated below. You do not have to sign this form to be eligible for TANF, SNAP, or Medicaid. However, you must sign this form if you want to be eligible for an exemption from the employment services program.
I authorize |
|
to complete Form |
|
|
|
|
Doctor, Medical Facilities or other Health Care Providers |
release the information to HHSC and the Texas Workforce Commission for purposes of verifying the medical condition that prevents me from
participating fully in the employment services program. This authorization expires on |
. |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Client or Personal Representative's Signature |
|
|
|
Date |
If you are signing for the client, please describe your authority to act for the client: |
|
|
|
|
|
Note: If the person requesting the release of case information cannot sign his/her name, two witnesses to his/her mark (X) must sign below:
Witness |
Date |
Witness |
Date |
Notice to Client
HHSC, as receiver of this information, will protect your personal health information in accordance with federal and state privacy regulations. If you authorize release of your health information to other parties, it may no longer be protected by privacy regulations.
You can withdraw permission you have given your doctor or health care provider to use or disclose health information that identifies you, unless they have already taken action based on your permission. You must withdraw your permission in writing.
Form Data
| Fact Name | Detail |
|---|---|
| Form Identification | Medical Release/Physician's Statement Form H1836-A |
| Release Date | March 2015-E |
| Sections in Form | Three sections: To Be Completed By Staff, To Be Completed By Physician, To Be Completed By Patient or Patient's Personal Representative |
| Primary Purpose | To verify a patient's physical or mental incapability of working for benefits eligibility. |
| Regulating Bodies | Managed by the Health and Human Services Commission (HHSC) with provisions for Federal and state regulations. |
| Assessment Areas | Includes assessment of personal disability, activity restrictions, and diagnosis. |
| Physician Responsibilities | Physicians are required to accurately detail the patient's ability to work, restrictions, and diagnosis. |
| Patient Authorization | Patients must authorize the release of medical information for employment services program exemption. |
| Privacy Notice | Advises on the protection of personal health information in accordance with federal and state privacy regulations. |
Instructions on Utilizing H1836 A
Filling out the H1836-A form is a necessary step for individuals applying for certain benefits who are claiming a disability that prevents them from working or participating in work-related activities. This form requires detailed information from both the applicant and their physician. It is designed to assess the applicant's ability to work and any restrictions they may have. Accuracy and thoroughness are key when completing this form, as it will significantly impact the assistance provided. Following the prescribed steps to fill out this form ensures that all necessary information is communicated effectively.
- Section I - To Be Completed By Staff:
- Enter the patient's name, date of birth, and Social Security Number.
- Fill in the case name (caregiver) and case number.
- Provide the patient's usual job.
- List the Health and Human Services Commission (HHSC) office address, HHSC mail code, and HHSC fax number.
- Section II - To Be Completed By Physician:
- Review the information provided by the staff in Section I to verify the patient's details.
- In Part A, select the appropriate level of the patient's ability to work or participate in work-related activities. If there are restrictions, indicate them and complete Parts B and C as applicable.
- In Part B, check the boxes that match the individual's activity restrictions during a workday, including sitting, standing, walking, and more.
- In Part C, list the primary and secondary disabling diagnoses. Provide any further comments, recommendations, or restrictions that could aid in understanding the patient's condition.
- Complete the physician's information, including name, signature, license number, office address, and phone number.
- Section III - To Be Completed By Patient or Patient's Personal Representative:
- Enter the patient's name to authorize the release of medical information necessary for verifying the medical condition that limits participation in the employment services program.
- Sign and date the form to provide consent. If you are the patient's personal representative, describe your authority to act for the patient.
- If the patient cannot sign their name, ensure two witnesses sign the form after the patient’s mark (X).
After completing the form as directed, the next step involves submitting it to the HHSC. Ensure that all parts of the form are filled out correctly and in entirety. A physician may hand the form back to the patient or choose to mail it directly to the HHSC. It is imperative that the form is submitted timely to avoid any delays in the evaluation process. Remember, this document plays a crucial role in determining eligibility for benefits, emphasizing the importance of accuracy and clarity in every section.
Obtain Answers on H1836 A
What is Form H1836-A?
Form H1836-A, known as the Medical Release/Physician's Statement, is a document used by the Texas Health and Human Services Commission (HHSC). It is designed for patients applying for benefits, such as TANF, SNAP, or Medicaid, who claim a physical or mental incapacity that prevents them from working or participating in work-related activities. This form must be completed by a physician to verify the patient's health condition and work capability.
Who needs to complete Form H1836-A?
Form H1836-A must be filled out by two main parties: The first part is completed by the staff of the Health and Human Services Commission, which includes the patient's details. The second and critical part of the form is to be filled out by the physician who assesses and verifies the patient's disability, specifying whether the individual can work and, if so, under what restrictions.
How does a physician complete Form H1836-A?
In completing Form H1836-A, a physician is required to provide an expert assessment of the patient's ability to work or participate in activities geared toward employment preparation. This involves checking appropriate boxes to indicate the patient's work capability, noting any specific restrictions, and providing a diagnosis. Additionally, the physician must offer opinions on the patient's capability to engage in less physically demanding activities or employment-related activities within a classroom setting.
Is Form H1836-A mandatory for all benefit applicants?
No, Form H1836-A is not required for all benefit applicants. It is specifically for those who claim a physical or mental condition that prevents them from working or participating in work-related activities. Signing this form is essential for applicants seeking an exemption from the employment services program as part of their benefits application.
What happens after Form H1836-A is completed?
Once Form H1836-A is filled out by the physician, it can either be given back to the patient or mailed directly to the HHSC at the provided address. The information provided will then be used by HHSC to determine the patient's eligibility for an exemption from work requirements as part of their benefits application. It is essential that the form is completed accurately to ensure a fair assessment of the patient's condition and capabilities.
Can a patient refuse to authorize the release of medical information?
Yes, patients have the right to refuse to sign Form H1836-A, thus not authorizing the release of their medical information for the purposes of verifying their incapacity to work. However, it's important to note that while refusal does not affect their eligibility for TANF, SNAP, or Medicaid benefits, it may affect their eligibility for exemptions from the employment services program. Patients wishing to withdraw previously granted authorization must do so in writing.
Common mistakes
When filling out the H1836 A form, a Medical Release/Physician's Statement, several mistakes can occur due to oversight or misunderstanding. Recognizing and avoiding these mistakes ensures the information is accurately and completely provided, facilitating a smooth process. Here are ten common mistakes:
- Not verifying patient information: Failing to double-check the patient's name, date of birth, and Social Security number can lead to processing delays.
- Incomplete case information: Leaving out the case name or case number can prevent the form from being matched with the correct file.
- Skipping physician's contact details: Not providing the physician's name, license number, or office contact information can hinder HHSC's ability to verify the form.
- Not specifying work capability: Failing to check one of the boxes under Part A to indicate the patient's ability to work or participate in preparatory activities.
- Omitting details in Part B (Activity Restrictions): Not specifying the patient's physical limitations in detail leaves an incomplete picture of their condition.
- Leaving Part C (Diagnosis) blank: Not including a primary or secondary disabling diagnosis omits critical information needed for evaluating the patient's eligibility for benefits.
- Unclear authorization: Patients or their representatives not signing the authorization section can prevent HHSC from obtaining the necessary medical records.
- Misunderstanding the form's purpose: Some might not realize that not signing the form could affect their eligibility for an exemption from employment services.
- Assuming temporary conditions don't qualify: Not indicating conditions that are expected to last more than 6 months because they believe only permanent disabilities are relevant.
- Forgetting to specify the expiration date of authorization: Not filling in the expiration date for the release of medical information can cause administrative issues.
Ensuring the form is accurately completed helps expedite the application process, reducing potential delays in receiving benefits or services. Attention to detail and providing thorough, precise information are key.
Documents used along the form
When processing or applying for certain benefits and exemptions through health and social service programs, the H1836-A form—known as the Medical Release/Physician's Statement—is a critical document that establishes a person's medical inability to work or participate in preparation for work activities due to physical or mental incapacity. However, this form often does not stand alone in the application process. There are several other forms and documents frequently required to supplement the information provided in the H1836-A, ensuring a comprehensive evaluation of an individual's eligibility and needs.
- Form H1010: Texas Health and Human Services Application for Assistance - This general application form is utilized to apply for a variety of assistance programs, including SNAP (food benefits), TANF (cash assistance for families), and Medicaid. It gathers personal, financial, and household information to determine basic eligibility for assistance.
- Form H1028: Employment Verification - A form used to verify a person's employment status, hours worked, and income. It provides essential information when assessing the need for an employment-related exemption due to medical conditions.
- Form H1033: Notice of Privacy Practices Acknowledgment - This document must be signed by applicants to acknowledge that they have received a notice of privacy practices, explaining how their medical information may be used and disclosed by health and human services programs.
- Form H1200: Application for Aged and Disabled Medicaid - Specifically designed for elderly and disabled individuals seeking Medicaid benefits, this form requires detailed information on medical conditions, treatments, and any disabilities that may affect work ability.
- Form SS-5: Application for a Social Security Card - While not directly related to health services, obtaining or updating a Social Security card is often a prerequisite for eligibility verification for various assistance programs.
- Form I-9: Employment Eligibility Verification - Necessary for individuals who are employed and seeking exemptions based on their medical condition, this form verifies an individual's eligibility to work in the United States, aligning with certain program requirements.
- Medical Records: Official documentation from hospitals, clinics, and other healthcare providers detailing an individual's medical history, diagnoses, and treatments. These records complement the physician's statement on the H1836-A by providing a more detailed account of the medical condition.
Collectively, these documents ensure a thorough and fair assessment of an individual's situation, addressing both the medical and socio-economic aspects that contribute to their eligibility for benefits and exemptions. Together with the H1836-A form, they form a comprehensive dossier that health and human services personnel use to make informed decisions that best support the needs and well-being of applicants.
Similar forms
The SSA-827 (Authorization to Disclose Information to the Social Security Administration) is quite similar to the H1836-A form because both documents require the individual's authorization to release medical information to a government agency. These forms serve as a bridge between the patient's medical records and the governmental body, ensuring the agency has the necessary information to make informed decisions regarding benefits or services.
The Form I-693 (Report of Medical Examination and Vaccination Record) shares similarities in the sense that it also involves a health professional providing detailed information about an individual's health status. However, the I-693 is specifically used for immigration purposes, verifying an immigrant’s health to ensure public safety and compliance with vaccination requirements.
The HIPAA Authorization Form parallels the H1836-A in terms of privacy considerations. Both documents require the individual's explicit consent to release health information, but the HIPAA Authorization Form is more general, applying to various health care scenarios beyond the government benefits context.
The VA Form 21-4142 (Authorization and Consent to Release Information to the Department of Veterans Affairs) is designed for veterans to consent to the release of their medical and other information to the VA. This form is similar because it directly concerns the relationship between an individual’s health condition and their eligibility for certain benefits or programs.
Medicare Authorization to Disclose Personal Health Information form is structured to allow release of personal health information by Medicare beneficiaries. Like the H1836-A, its principal function is to ensure relevant health information can be shared with entities needing it to provide benefits or services.
The Form DS-3025 (Vaccination Documentation Worksheet) is used in the immigration process, akin to Form I-693, but focuses more narrowly on the vaccination status of the applicant. Its similarity comes from the physician's role in verifying medical conditions and capabilities, albeit for a different purpose.
A Worker’s Compensation Release Form is another document that overlaps with the H1836-A in its utility to ascertain an individual’s capacity to work following an injury. These forms help determine eligibility for benefits by assessing the physical or mental ability of a person to engage in employment.
The Disability Benefits Forms from various insurance companies often require a physician’s statement similar to the H1836-A, assessing the extent of an individual's disability and their ability to work. These forms facilitate the processing of claims based on the medical condition of the claimant.
The Consent to Participate in a Program form, often used in educational and rehabilitation settings, might not directly concern medical information but similarly requires documentation of an individual's condition and capabilities, making it somewhat parallel to the H1836-A’s intent of documenting limitations for program participation.
Dos and Don'ts
When filling out the H1836 A form, it is crucial to adhere to specific dos and don'ts to ensure that the process is completed accurately and efficiently. Below is a guide on the things you should and shouldn't do when working with this form:
Things You Should Do
Ensure that all sections required by your role are filled out completely. For patients or their representatives, this includes the authorization in Section III. Physicians must complete Section II thoroughly.
Review the instructions carefully before starting to fill out the form. This ensures that all necessary details are included and correctly entered.
Provide precise and accurate medical information, especially in the diagnosis and activity restriction areas. This information is crucial for assessing eligibility for employment service program exemptions.
Use black or blue ink if filling out the form by hand to ensure legibility and to prevent any issues with photocopying or scanning the document.
Keep a copy of the completed form for your records before submitting it to the Health and Human Services Commission (HHSC) or providing it to the patient.
Things You Shouldn't Do
Do not leave any required fields blank. If a specific question does not apply, indicate with an "N/A" (not applicable) rather than leaving the space empty.
Avoid using medical jargon that may not be easily understood by non-medical personnel processing the form. Instead, aim for clear and concise terms whenever possible.
Refrain from guessing information when unsure. If necessary, seek clarification or additional information to ensure accuracy.
Do not submit the form without the patient's or personal representative’s signature in Section III if the patient is applying for an exemption from the employment services program.
Avoid making alterations or using correction fluid on the form. If errors are made, it is better to start with a new form to maintain neatness and legibility.
Misconceptions
One common misconception is that the H1836-A form can only be completed by doctors. In fact, the form clearly states it can be completed by physicians, which includes a broader range of medical professionals such as specialists and psychiatrists, not just general practitioners.
Another misconception is that the form is only related to physical disabilities. However, the form also accommodates mental and psychological disabilities. It asks for the primary and secondary disabling diagnosis, which indicates that it covers a wide range of disabilities beyond just physical ones.
Some people believe that if a patient can work at all, they cannot use this form to request an exemption from work requirements. Yet, the form clearly provides options for individuals who can work with restrictions, indicating that partial ability does not disqualify one from seeking an exemption.
There's also a belief that this form automatically qualifies you for disability benefits. This is not accurate. The H1836-A form is used to verify a medical condition for exemption from employment services programs, not to grant disability benefits. Other processes and documentation are required for disability benefit applications.
A misconception exists that signing the H1836-A form will make one's health information public. In reality, the notice to the client section emphasizes that HHSC will protect personal health information according to federal and state privacy regulations. Only authorized entities will have access to this information for the specified purposes.
Finally, some believe that once signed, the authorization to release medical information on the form is irrevocable. However, the form explicitly states that clients can withdraw their permission in writing unless action has already been taken based on that permission, showing that clients have control over their medical information.
Key takeaways
When dealing with the Medical Release/Physician's Statement Form H1836-A, it's crucial to understand its components and the procedures for completing and using it appropriately. This understanding ensures compliance with federal and state regulations, particularly for individuals applying for benefits who are unable to work due to physical or mental incapabilities. Here are key takeaways to guide patients, caregivers, and healthcare providers through this process:
- The Form H1836-A is essential for individuals applying for benefits who claim a disability that prevents them from working or participating in work preparation activities.
- Section I of the form should be filled out by staff, including details about the patient, such as their name, date of birth, social security number, and case information.
- Physicians must complete Section II, providing vital information about the patient's ability to work or participate in work-preparation activities, including the extent of any restrictions and the nature of the disability.
- The form offers options to indicate whether an individual can work without restrictions, with restrictions, or is unable to work at all. This distinction is critical for the proper assessment of the patient's eligibility for exemptions from employment services programs.
- Part B and Part C within Section II allow the physician to detail the patient's activity restrictions and provide a diagnosis, underscoring the importance of a comprehensive medical evaluation.
- In Section III, the patient or patient's personal representative authorizes the release of medical information, granting permission for HHSC and the Texas Workforce Commission to verify the medical condition in question.
- It's imperative to note that signing this authorization is not mandatory for eligibility for most benefits but is required for an exemption from the employment services program. Additionally, the form includes a clause about the protection of personal health information, in line with federal and state privacy regulations.
Understanding and accurately completing the Form H1836-A is vital for both applicants seeking benefits and the professionals assisting them. It not only ensures the integrity of the application process but also the well-being of those genuinely in need of support due to their inability to work. Physicians play a key role in providing detailed and accurate information about the patient's condition, which is essential for determining eligibility for benefit programs and potential exemptions.
Popular PDF Forms
Separation Notice - Employers are required to clarify whether the separation was due to lack of work or other reasons, providing full details if it's the latter.
Ar 600–8–2 - It helps document the completion date of any punishment or adverse action.
Mvr-615 - Eligibility for automobile insurance in North Carolina for a non-fleet private passenger vehicle is determined using the criteria listed in the MVR-615 form.