Blank Individual Service Plan Wisconsin PDF Template
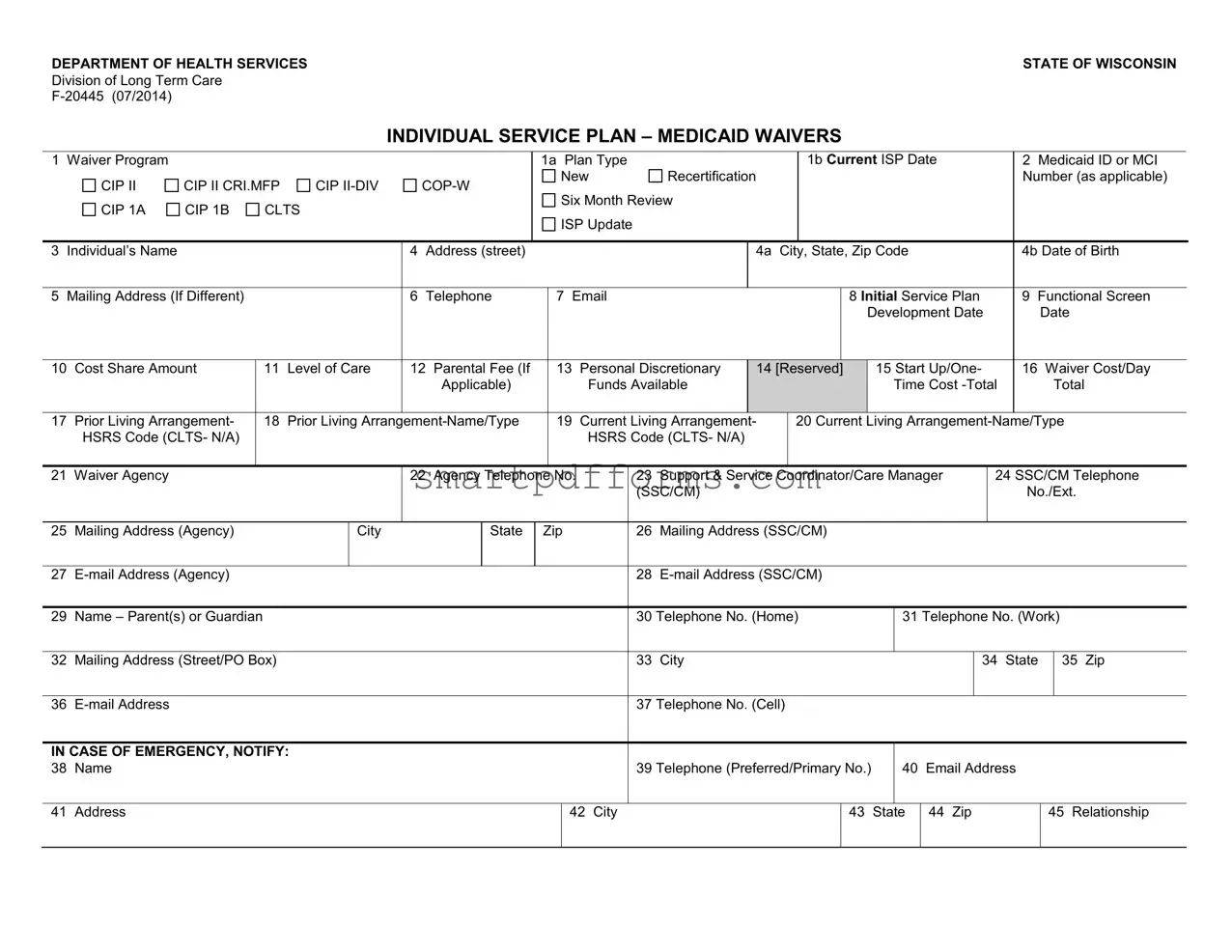
The Individual Service Plan (ISP) in Wisconsin plays a critical role in supporting residents who qualify for Medicaid waivers, enabling them to receive various services based on their specific needs. This meticulous document, outlined by the Department of Health Services, is crucial for implementing personalized care and assistance that cater to individual requirements. The plan covers an extensive array of details including the type of waiver program, Medicaid identification, the current plan and review dates, as well as personal information about the individual such as their name, address, and contact details. It delves into the realms of care levels, financial aspects like cost-sharing and parental fees, and living arrangements prior to and post the initiation of the plan. Agencies and coordinators involved in providing support are clearly identified, ensuring an organized and systematic approach to care. Detailed within the plan are specific services, including codes, names, providers, costs, and the intended outcomes, establishing a structured approach to managing and delivering care services. Importantly, the plan emphasizes the individual’s right to informed choices - from choosing between community services and nursing homes to selecting service types and providers. Updates, signature requirements, and variance requests for particular living arrangements underscore the document's comprehensive nature, embodying the commitment to informed, personalized, and dignified care for Wisconsin's Medicaid waiver recipients.
Preview - Individual Service Plan Wisconsin Form

DEPARTMENT OF HEALTH SERVICESSTATE OF WISCONSIN
Division of Long Term Care
INDIVIDUAL SERVICE PLAN – MEDICAID WAIVERS
1 Waiver Program |
|
|
|
|
|
|
|
|
1a Plan Type |
|
|
|
|
|
1b Current ISP Date |
|
|
|
|
2 Medicaid ID or MCI |
|
||||||||||||
|
CIP II |
CIP II CRI.MFP |
CIP |
|
|
New |
|
Recertification |
|
|
|
|
|
|
|
|
|
|
|
|
Number (as applicable) |
|
|||||||||||
|
|
|
Six Month Review |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
CIP 1A |
CIP 1B |
CLTS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
ISP Update |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
Individual’s Name |
|
|
|
|
|
4 |
Address (street) |
|
|
|
|
|
|
|
4a |
City, State, Zip Code |
|
|
|
|
|
4b Date of Birth |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
5 |
Mailing Address (If Different) |
|
|
|
6 |
Telephone |
|
7 |
|
|
|
|
|
|
8 Initial Service Plan |
|
9 Functional Screen |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Development Date |
|
|
Date |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
10 |
Cost Share Amount |
|
11 |
Level of Care |
12 Parental Fee (If |
|
13 |
Personal Discretionary |
14 [Reserved] |
|
15 Start Up/One- |
|
16 Waiver Cost/Day |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
Applicable) |
|
|
|
Funds Available |
|
|
|
|
|
|
|
Time Cost |
|
|
|
Total |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
17 |
Prior Living Arrangement- |
|
18 |
Prior Living |
|
19 |
Current Living Arrangement- |
|
20 Current Living |
|
|||||||||||||||||||||||
|
HSRS Code (CLTS- N/A) |
|
|
|
|
|
|
|
|
|
|
HSRS Code (CLTS- N/A) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
21 |
Waiver Agency |
|
|
|
|
|
22 Agency Telephone |
No. |
|
23 |
Support & Service |
Coordinator/Care Manager |
|
|
24 SSC/CM Telephone |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(SSC/CM) |
|
|
|
|
|
|
|
|
|
|
|
|
|
No./Ext. |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
25 |
Mailing Address (Agency) |
|
|
City |
|
|
State |
Zip |
|
|
26 |
Mailing Address (SSC/CM) |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
27 |
|
|
|
|
|
|
|
|
|
|
|
28 |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
29 |
Name – Parent(s) or Guardian |
|
|
|
|
|
|
|
|
|
|
|
30 |
Telephone No. (Home) |
|
31 Telephone No. (Work) |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
32 |
Mailing Address (Street/PO Box) |
|
|
|
|
|
|
|
|
|
|
33 |
City |
|
|
|
|
|
|
|
|
|
|
34 |
State |
35 Zip |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
36 |
|
|
|
|
|
|
|
|
|
|
|
|
|
37 |
Telephone No. (Cell) |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
IN CASE OF EMERGENCY, NOTIFY: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
38 |
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
39 |
Telephone (Preferred/Primary No.) |
|
40 |
Email Address |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
41 |
Address |
|
|
|
|
|
|
|
|
|
|
42 City |
|
|
|
|
|
43 |
|
State |
44 |
Zip |
|
|
45 Relationship |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
62 Service Code #
63 Service Name
64 |
65 |
Outcome No. |
Service Provider Name Address and |
Telephone No. |
|
|
(Email, cell phone no., if known) |
65a
Start Date
65b
End Date
66
Unit Cost ($/hr; day)
67
Authorized Units of Service and Frequency
(#/day or week or month)
68 |
69 |
Daily Cost (total |
Funding |
yearly ÷ 365 days) |
Source |
|
|

70 PARTICIPANT INFORMED – R IGHTS AND CHOICE (Review REQUIRED at initial plan development and recertification.)

 I have been informed that I have a RIGHT TO CHOOSE between a nursing home or
I have been informed that I have a RIGHT TO CHOOSE between a nursing home or

 I have been informed of my CHOICES in the waiver programs, including my right to CHOOSE the TYPE OF SERVICES I receive under my service plan.
I have been informed of my CHOICES in the waiver programs, including my right to CHOOSE the TYPE OF SERVICES I receive under my service plan.

 I understand that I have CHOICES in the waiver programs, including my right to CHOOSE from available, qualified providers that will provide the services outlined in my plan.
I understand that I have CHOICES in the waiver programs, including my right to CHOOSE from available, qualified providers that will provide the services outlined in my plan.

 I have been informed verbally and in writing of my rights and responsibilities in the Medicaid Waiver Programs and I understand these rights and responsibilities.
I have been informed verbally and in writing of my rights and responsibilities in the Medicaid Waiver Programs and I understand these rights and responsibilities.

 I have been informed verbally and in writing of my RIGHT TO REQUEST A HEARING should I disagree with decisions made about my ELIGIBILITY to participate in the HCBS program.
I have been informed verbally and in writing of my RIGHT TO REQUEST A HEARING should I disagree with decisions made about my ELIGIBILITY to participate in the HCBS program.

 I have been informed verbally and in writing of my RIGHT TO REQUEST A HEARING should I disagree with decisions made that would DENY, REDUCE OR TERMINATE the services I receive.
I have been informed verbally and in writing of my RIGHT TO REQUEST A HEARING should I disagree with decisions made that would DENY, REDUCE OR TERMINATE the services I receive.

 By my signature below I indicate I have chosen to accept community services through a Medicaid Home and Community Waiver Program.
By my signature below I indicate I have chosen to accept community services through a Medicaid Home and Community Waiver Program.
71 UPDATE/REVIEW VERIIFICATION - APPLIES TO PLAN REVIEW OR ISP UPDATE ONLY

 The SIX MONTH ISP Review was completed with the participant/guardian on the date below and there are no changes to the ISP at this time.
The SIX MONTH ISP Review was completed with the participant/guardian on the date below and there are no changes to the ISP at this time.

 The SIX MONTH ISP Review was completed with the participant/guardian on the date below and agreed upon changes to the ISP are included herein.
The SIX MONTH ISP Review was completed with the participant/guardian on the date below and agreed upon changes to the ISP are included herein.

 The ISP was UPDATED on the date below to reflect changes (additions, increases or reductions) to planned services or providers or to units/frequency of service.
The ISP was UPDATED on the date below to reflect changes (additions, increases or reductions) to planned services or providers or to units/frequency of service.
SIGNATURES: ISP Signature Requirements apply at the time of plan development, review and recertification.
SIGNATURE - Participant |
Date Signed |
SIGNATURE – Support and Service Coordinator/Care Manager |
Date Signed |
|
|
|
|
SIGNATURE – Guardian/Authorized Representative/Parent |
Date Signed |
SIGNATURE - Guardian/Authorized Representative/Parent |
Date Signed |
|
|
|
|
SIGNATURE - Witness |
Date Signed |
SIGNATURE – Witness |
Date Signed |
|
|
|
|
DISTRIBUTION: Original – DHS; Copy - County Care Manager/Support and Service Coordinator; Copy – Individual; Copy - Authorized Representative

CIP

 A variance to the
A variance to the

 A variance to allow waiver funding for an individual that is elderly to reside in a CBRF connected to a nursing home
A variance to allow waiver funding for an individual that is elderly to reside in a CBRF connected to a nursing home
BY SIGNING BELOW, THE SUPPORT AND SERVICE COORDINATOR / CARE MANAGER ATTESTS TO THE FOLLOWING:
1.The environment is
2.The facility is the preferred residence of the applicant/participant or his/her legal representative.
SIGNATURE - Participant |
Date Signed |
SIGNATURE – Support and Service Coordinator/Care Manager |
Date Signed |
|
|
|
|
SIGNATURE – Guardian/Authorized Representative/Parent |
Date Signed |
SIGNATURE - Guardian/Authorized Representative/Parent |
Date Signed |
|
|
|
|
SIGNATURE - Witness |
Date Signed |
SIGNATURE – Witness |
Date Signed |
|
|
|
|
DISTRIBUTION: Original – DHS; Copy - County Care Manager/Support and Service Coordinator; Copy – Individual; Copy - Legal Representative
Form Data
| Fact Name | Description |
|---|---|
| Form Title | Individual Service Plan – Medicaid Waivers |
| Form Number | F-20445 (07/2014) |
| Issuing Department | Department of Health Services, State of Wisconsin, Division of Long Term Care |
| Purpose | To outline the services and supports provided to individuals under Medicaid Waivers in Wisconsin. |
| Key Sections | Waiver Program, Individual's Information, Cost Share and Level of Care, Support & Service Coordination, Rights and Choices, Signature Requirements |
| Governing Laws | Medicaid Waivers under the Wisconsin State Statutes and Regulations. |
| User Audience | Individuals receiving Medicaid Waiver services, their guardians or authorized representatives, and care managers or coordinators. |
| Signature Requirements | Required at the time of plan development, review, and recertification from the participant, Support and Service Coordinator/Care Manager, Guardian/Authorized Representative/Parent, and Witness. |
| Emergency Contact Information | Includes a section for detailing emergency contact information, highlighting the form's comprehensive nature in planning for the individual's wellbeing. |
| Update/Review Verification | Specifies the process for six-month reviews and updates, ensuring the plan remains relevant and responsive to the individual's needs. |
Instructions on Utilizing Individual Service Plan Wisconsin
Filling out the Individual Service Plan (ISP) for Medicaid Waivers in Wisconsin is a critical step for individuals to receive customized services that best meet their needs. This plan outlines the types of support and services an individual requires, acknowledges their preferences, and defines the goals aimed at enhancing their quality of life while maintaining their independence in the community. To ensure the process is smooth and efficient, follow these detailed steps closely.
- Identify the Waiver Program and mark the appropriate box at the top of the form.
- Choose the Plan Type by selecting either "New," "Recertification," "Six Month Review," or "ISP Update."
- Enter the Current ISP Date if applicable.
- Fill in the individual's Medicaid ID or MCI Number as required.
- Provide the Individual’s Name and complete details like Address, City, State, Zip Code, and Date of Birth.
- If different, include a Mailing Address along with Telephone and Email contact information.
- Mark the checkbox for Initial Service Plan if this is the first time the plan is being developed.
- Enter the Functional Screen Development Date.
- Fill out financial information including Cost Share Amount, Level of Care, and Parental Fee if applicable.
- List any Personal Discretionary Funds Available.
- Detail the Start Up/One-Time Cost - Total Waiver Cost/Day.
- Describe Prior and Current Living Arrangements with associated HSRS Code if applicable.
- Include information for the Waiver Agency and Support & Service Coordinator/Care Manager including telephone numbers, mailing addresses, and email addresses.
- Under "IN CASE OF EMERGENCY," provide contact information including Name, Telephone, Email Address, and Address of the emergency contact and their Relationship to the individual.
- For service details, enter each Service Code, Service Name, and Service Provider information including contact details, Start and End Dates, Unit Cost, and Authorized Units of Service and Frequency.
- Calculate and enter the Daily Cost and state the Funding Source.
- Acknowledge the section on PARTICIPANT INFORMED – RIGHTS AND CHOICE indicating that the participant has been fully informed of their rights and has made informed choices about their service plan. The participant or their representative must sign this section.
- If the form is for UPDATE/REVIEW VERIFICATION, indicate whether it's a scheduled review or an update due to changes and provide the relevant dates.
- Ensure all SIGNATURES required at the time of plan development, review, or recertification are signed by the relevant parties: the participant, Support and Service Coordinator/Care Manager, Guardian/Authorized Representative/Parent, and witnesses.
- Adhere to the DISTRIBUTION instructions at the bottom of the form to ensure all parties receive a copy of the ISP.
Once completed, the form will serve as a comprehensive plan tailored to meet the individual’s specific needs, ensuring they receive the appropriate supports and services to live safely and comfortably within their community. Remember, thorough and accurate completion of this form is essential for the effective implementation of services and support.
Obtain Answers on Individual Service Plan Wisconsin
What is the Individual Service Plan (ISP) in Wisconsin?
The Individual Service Plan (ISP) in Wisconsin is a document designed under the Medicaid Waivers program. It outlines the personalized services and supports each participant receives to meet their specific health and independent living needs. The ISP covers various aspects such as the type, frequency, and providers of services.
Who needs to complete the Individual Service Plan?
This plan must be completed for individuals who are participating in Medicaid Home and Community-Based Service Programs in Wisconsin. It involves collaboration between the participant, their family or guardian, and their Support and Service Coordinator or Care Manager.
What information is included in the ISP?
The ISP includes details such as the waiver program type, plan type, Medicaid ID, service codes, service names, service providers, cost share amounts, and levels of care. It also records the participant's living arrangements, waiver agency information, and emergency contacts.
How often is the ISP reviewed or updated?
The plan is subject to review at least every six months. However, it may also be updated more frequently as needed to reflect changes in the participant's service needs or living situation.
What rights do participants have regarding their ISP?
Participants have the right to choose between nursing home or community services, select the types of services they receive, choose their service providers from available qualified candidates, and be informed of their rights and responsibilities. They also have the right to request a hearing if they disagree with decisions made about their eligibility or the services they receive.
What is required for the ISP signature?
Signatures are required from the participant, their Support and Service Coordinator/Care Manager, and their guardian or authorized representative, if applicable, at the time of plan development, review, and recertification.
How are ISP documents distributed?
After signing, the original ISP document is sent to the Department of Health Services (DHS), while copies are distributed to the County Care Manager or Support and Service Coordinator, the individual, and their authorized representative.
Can the ISP be modified?
Yes, the ISP can be modified during the six-month review or as needed to accurately reflect changes in the participant's needs or preferences for services and supports.
What happens if a participant disagrees with decisions related to the ISP?
Participants who disagree with decisions regarding their eligibility, the denial, reduction, or termination of services have the right to request a hearing. They are informed of this right both verbally and in writing.
Common mistakes
When filling out the Individual Service Plan (ISP) for Medicaid Waivers in Wisconsin, it's crucial to avoid common mistakes for accurate and successful submission. Here are eight frequent errors that people should watch out for:
Not specifying the Waiver Program type: The form requires indicating whether it’s a new plan, recertification, or a six-month review. Overlooking this detail can lead to processing delays.
Incorrect Medicaid ID or MCI number: This critical piece of information must be accurate. Any discrepancy between the provided information and official records can complicate or void the application process.
Leaving contact information sections incomplete: The form asks for various contact details, including telephone numbers and email addresses for the individual, parents, guardians, and emergency contacts. Failing to provide all required contact information can result in communication issues.
Omitting details about living arrangements: Both prior and current living situations must be thoroughly documented. Missing out on these details can affect the assessment of the individual's needs and eligibility.
Forgetting to list the support and service coordinator/care manager: Their contact information is vital for coordinating and managing the services provided. Neglecting to include it may disrupt service delivery.
Incomplete service information: Each requested service must include the service code, name, provider information, start and end dates, cost, and frequency. Incomplete information can lead to delays or denial of services.
Not acknowledging rights and choices: The individual's signature is required to confirm they have been informed about their rights and choices under the waiver programs. Missing signatures can lead to compliance issues.
Skipping the signature section: All necessary signatures from the participant, guardian or authorized representative, and the support and service coordinator/care manager are mandatory for the form’s validity. Overlooking this section renders the submission incomplete.
Avoiding these mistakes can significantly enhance the accuracy and efficiency of the Individual Service Plan process, ensuring that individuals receive the appropriate services to meet their needs.
Documents used along the form
When working with the Individual Service Plan (ISP) in Wisconsin, professionals often find themselves navigating through a variety of additional forms and documents. These documents are vital for ensuring comprehensive care and support for individuals receiving services through Medicaid waivers. Each serves a unique purpose, contributing to the holistic planning and implementation of personalized care.
- Functional Screen: A detailed assessment that evaluates an individual’s need for long-term support, determining eligibility for various programs and services.
- Emergency Contact Information: A form providing contact information for individuals to be notified in case of an emergency, critical for immediate response and care coordination.
- Medical Information Form: Documents an individual’s medical history, current medications, and healthcare providers, ensuring all care team members have access to vital health information.
- Consent for Release of Information: Authorizes the sharing of specified health and personal information between agencies and providers, facilitating coordinated support and services.
- Financial Information Form: Collects information on an individual’s financial resources, necessary for determining program eligibility and cost-sharing responsibilities.
- Service Agreement: A contract between the service provider and the recipient, detailing the services to be provided, expected outcomes, and terms of service.
- Guardianship or Power of Attorney Documents: Legal documents that identify the individual or entity authorized to make decisions on behalf of the participant, crucial for informed care and support.
- Behavior Support Plan: For individuals with behavioral challenges, this plan outlines strategies and interventions for managing behavior, promoting positive outcomes and safety.
- Health and Safety Plan: Identifies potential risks to the individual’s health and safety and outlines preventive measures and responses to emergencies.
- Service Provider Information: Information about agencies and individuals providing care and services, including qualifications, contact information, and service descriptions.
Comprehending and utilizing these documents effectively is essential for service coordinators, care managers, and other professionals supporting individuals through Medicaid waivers in Wisconsin. Each document plays a crucial role in ensuring that individuals receive tailored, high-quality care and support, addressing their unique needs and preferences. Integrating these documents with the ISP process enhances the coordination and delivery of services, ultimately contributing to better outcomes for individuals and their families.
Similar forms
504 Plan: Like the Individual Service Plan (ISP) in Wisconsin, a 504 Plan is designed to provide accommodations and support to individuals with disabilities, particularly in educational settings. While the 504 Plan focuses on ensuring students have equal access and opportunities to participate in school activities and coursework, the ISP aims to provide a broad range of services and support for individuals with disabilities to live more independently. Both plans are tailored to the individual's specific needs, involving a documented process and periodic reviews.
Individualized Education Program (IEP): An IEP is similar to the ISP as both are planning documents for individuals with disabilities. An IEP, used within the school system, aims to outline educational goals, services, and accommodations for children with disabilities. The ISP, while broader, focuses on a range of services beyond education, including living arrangements and community participation. Both plans are personalized, require regular assessments, and involve collaboration among professionals and the individual's family or guardians.
Treatment Plan: Treatment Plans in healthcare settings share similarities with the ISP form by offering personalized care strategies for individuals receiving medical or therapeutic services. Both documents outline specific goals, interventions, and the roles of various service providers. However, while Treatment Plans often focus on clinical and therapeutic goals within healthcare contexts, ISPs encompass a wider array of services aimed at supporting individuals in community-based settings.
Service Coordination Plan: Service Coordination Plans help manage and organize multiple services across different providers for individuals requiring comprehensive care. Like the ISP, they focus on ensuring that all aspects of an individual's care, including medical, educational, and social services, are coordinated seamlessly. Each plan is customized to the individual's needs, emphasizing holistic support.
Advanced Care Plan: This document, focusing on end-of-life care preferences, mirrors the individualized nature of the ISP. It outlines a person's wishes regarding healthcare and treatment in critical situations. Both plans highlight the importance of autonomy and informed choices in receiving care and services, though they serve different stages and contexts of an individual's life.
Personal Care Plan: Often developed in senior living or for individuals receiving in-home care, Personal Care Plans specify the services and support required for daily living, such as hygiene, nutrition, and mobility assistance. These plans share the ISP's goal of tailoring support to the individual's needs but typically focus more narrowly on personal care and less on broader community engagement or developmental goals.
Dos and Don'ts
When filling out the Individual Service Plan (ISP) for Medicaid Waivers in Wisconsin, it's essential to approach the task with care and attention to detail. Here are some dos and don'ts that can guide you through the process effectively:
Do:- Review all sections thoroughly before beginning to ensure you understand what information is required.
- Provide accurate and up-to-date information for every field, especially your contact details and Medicaid ID to ensure services are correctly allocated.
- Consult with a healthcare professional or care manager if you're unsure about the level of care needed or other specifics related to the service plan.
- Use clear and concise language to describe the desired outcomes and the specific services required to achieve those outcomes.
- Sign and date the form in all the required sections to validate the ISP. If a guardian or authorized representative is involved, ensure they also sign where necessary.
- Keep a copy of the completed form for your records and ensure that all other necessary parties receive their copies, as outlined in the distribution section of the form.
- Rush through the form without taking the time to consider each question's implications on the individual’s care and well-being.
- Leave sections incomplete, unless they are explicitly marked as optional or not applicable to your situation.
- Guess on specifics like service codes, cost share amounts, or level of care needed. Seek clarification when in doubt.
- Ignore the participant's rights and choice section. Understand your rights fully and communicate them clearly on the form.
- Forget to review and update the service plan as needed. The six-month review section is crucial for maintaining an accurate and effective plan.
- Overlook the requirement for review and verification signatures, including those of witnesses. These are crucial for the document’s validity.
Misconceptions
When it comes to the Individual Service Plan (ISP) form in Wisconsin, several misconceptions can lead to confusion for individuals and their families. Understanding these common misconceptions can help ensure that individuals receive the appropriate services and supports through Medicaid Waivers.
Misconception 1: Only individuals with physical disabilities are eligible for services.
In reality, the ISP covers a broad range of individuals, including those with intellectual and developmental disabilities, elderly individuals, and people with various types of chronic conditions or disabilities.Misconception 2: The ISP is a one-size-fits-all document.
Each ISP is uniquely tailored to the individual's specific needs, preferences, and goals. The plan is developed through a collaborative process involving the individual, their caregivers, and professionals.Misconception 3: Once the ISP is set, it can't be changed.
The document is flexible and subject to change whenever necessary. It includes provisions for regular reviews and updates to reflect any changes in the individual's needs or circumstances.Misconception 4: The individual has no say in the planning process.
Individuals have the right to actively participate in their service planning, including selecting services and providers, to the fullest extent possible.Misconception 5: All services are covered under the ISP.
While the ISP aims to cover a broad range of services and supports, there may be limitations based on Medicaid Waiver program rules and available funding.Misconception 6: Only the Support and Service Coordinator/Care Manager can initiate changes to the ISP.
The individual or their guardian/authorized representative can request changes to the plan at any time.Misconception 7: Signing the ISP document locks you into receiving services from a specific provider indefinitely.
Individuals have the right to choose their service providers and can change providers if they are not satisfied with the services received.Misconception 8: The ISP is only concerned with medical or health-related services.
It also encompasses supports for living arrangements, employment, personal care, and other areas critical to the individual's well-being and independence.Misconception 9: The ISP is only relevant for individuals in institutional settings.
The plan is designed to support individuals living in a variety of settings, including their own homes, community-based residential facilities, and other non-institutional environments.
Clear understanding and awareness of these misconceptions are vital for individuals and families navigating the complexities of Medicaid Waivers and seeking to maximize the benefits of the Individual Service Plan.
Key takeaways
Filling out the Individual Service Plan (ISP) in Wisconsin is a critical step for participants in Medicaid waiver programs. This guide highlights seven key takeaways to ensure the process is clear and beneficial for those involved.
- Understanding the Plan Types: The forms cater to different scenarios—new plans, recertification, six-month reviews, and updates. It’s important to identify which category the current process falls under to ensure that the ISP accurately reflects the participant's current needs and services.
- Participant Rights: Every participant has the right to choose between nursing home or community services, select the type of services received, and decide on their service providers from a list of qualified candidates. These rights underscore the participant’s autonomy in their care plan.
- Informed Decision-Making: Participants must be informed both verbally and in writing about their rights and responsibilities within the Medicaid Waiver Programs. This includes a clear understanding of the process to request a hearing if they disagree with decisions affecting their eligibility or the services provided.
- Comprehensive Information Required: The form requires detailed information, including Medicaid ID, current living arrangements, and contact details for the waiver agency and care managers. Accurate and complete information ensures the ISP is tailored to the participant's specific situation.
- Emergency Contact Details: Listing an emergency contact is essential. This contact will be notified in any urgent situations, making it critical to include someone reliable and available.
- Review and Update Verification: ISPs are living documents that require regular reviews and updates. The form captures whether the plan is at its initial creation, a six-month review, or if there are any updates, highlighting the process's ongoing nature aimed at reflecting the participant's evolving needs.
- Signatures for Verification: Signatures from the participant, guardian, or authorized representative, and the Support and Service Coordinator or Care Manager validate the plan. This formal acknowledgment ensures all parties agree with the documented plan and understand their roles and responsibilities.
Ensuring that the ISP form is filled out thoroughly and thoughtfully is crucial for facilitating appropriate and effective services tailored to the participant's needs. By keeping these key takeaways in mind, participants, guardians, and care managers can work together towards creating a plan that best supports the participant's goals and preferences within the Medicaid waiver programs.
Popular PDF Forms
Mental Health Treatment Plan Template - Geared towards rehabilitation psychologists, offering targeted treatment strategies to support client recovery and reintegration.
St 108 - The ST-108 reflects Indiana's commitment to fair tax practices in the automotive and boating industries.