Blank Mc 223 PDF Template
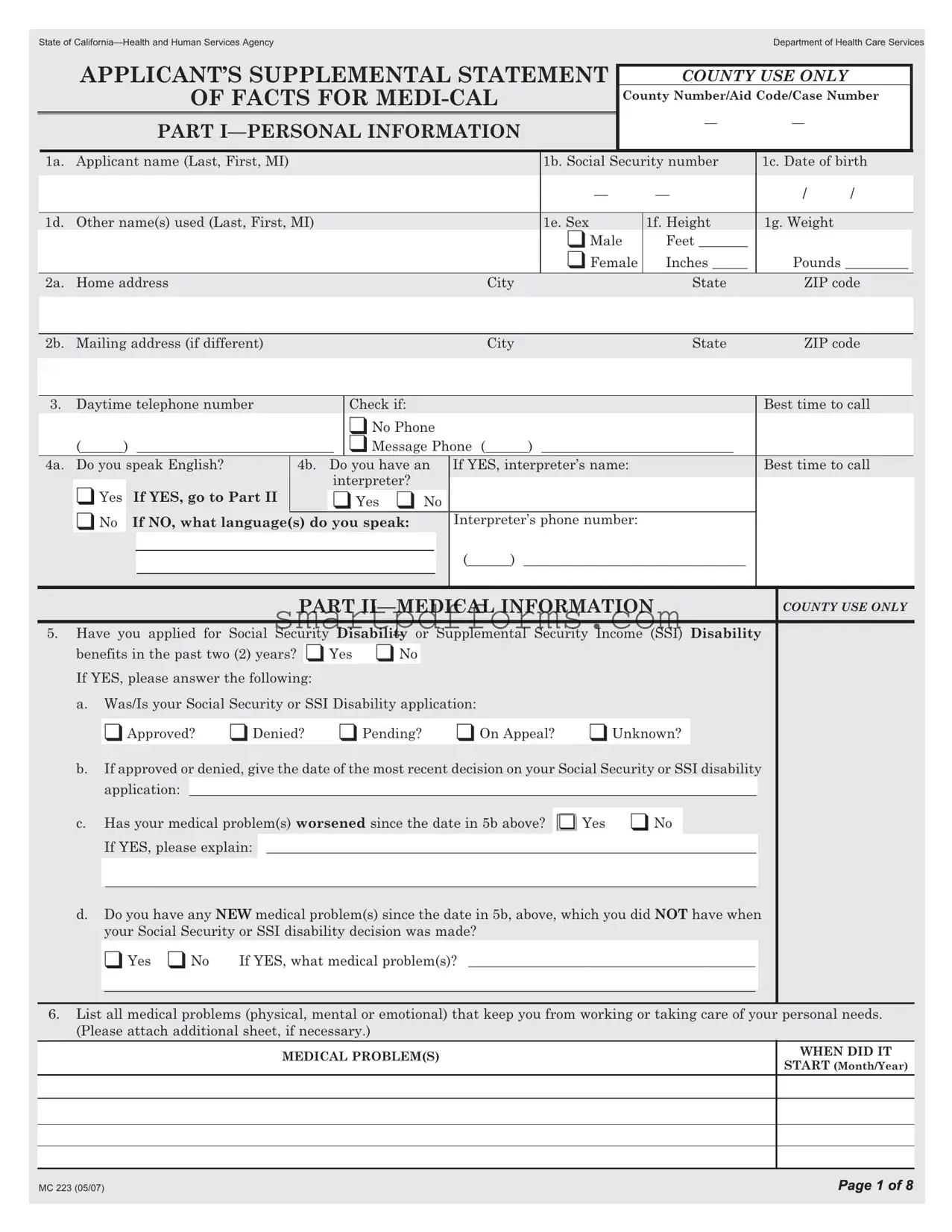
In navigating the complexities of accessing health services, particularly through programs like Medi-Cal in California, individuals encounter various forms of paperwork that are crucial for determining eligibility and the extent of benefits. Among these, the MC 223 form emerges as a critical document. Designed by the State of California—Health and Human Services Agency Department of Health Care Services, this comprehensive form serves as an Applicant's Supplemental Statement of Facts for Medi-Cal. It meticulously gathers personal information, including the applicant's name, Social Security number, and contact details, alongside medical information that paints a detailed picture of an individual's health status, disability claims, and healthcare history. Furthermore, it explores social and educational backgrounds, shedding light on how a person's daily life and capacities might be impacted by their medical conditions. Work history details are also solicited, providing insights into the nature and physical demands of an applicant's employment history. This exhaustive collection of data ensures that the evaluators have a holistic view of the applicant's circumstances, enabling a tailored assessment of their needs and entitlements under Medi-Cal. In essence, the MC 223 form is pivotal for applicants navigating the Medi-Cal program, bridging the gap between individual health needs and the provision of essential medical benefits.
Preview - Mc 223 Form
State of
|
|
APPLICANT’S SUPPLEMENTAL STATEMENT |
|
COUNTY USE ONLY |
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
OF FACTS FOR |
|
|
County Number/Aid Code/Case Number |
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
— |
— |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
PART |
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
1a. |
Applicant name (Last, First, MI) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1b. Social Security number |
|
1c. Date of birth |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
— |
— |
|
/ |
/ |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1d. |
Other name(s) used (Last, First, MI) |
|
|
|
|
|
|
|
|
|
|
|
|
|
1e. Sex |
1f. Height |
|
1g. Weight |
|
|
||||||||||
|
|
Home addressA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❑Male |
Feet _______ |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❑Female |
Inches _____ |
|
Pounds _________ |
|
||||||||||
|
2a. |
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
State |
ZIP code |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
2b. |
Mailing address (if different) |
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
State |
ZIP code |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
3. |
Daytime telephone number |
|
|
|
|
Check if: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Best time to call |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
❑No Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
( |
) |
|
|
|
|
|
|
❑Message Phone ( |
|
|
|
) |
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4a. |
Do you speak English? |
4b. |
Do you have an |
|
If YES, interpreter’s name: |
|
|
|
|
Best time to call |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
interpreter? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
❑Yes |
|
If YES, go to Part II |
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
❑Yes ❑ No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
❑No |
|
|
|
|
|
|
|
|
|
|
|
Interpreter’s phone number: |
|
|
|
|
|
|
|
||||||||||
|
|
If NO, what language(s) do you speak: |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
|
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PART |
COUNTY USE ONLY |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
5. |
Have you applied for Social Security Disability or Supplemental Security Income (SSI) Disability |
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
benefits in the past two (2) years? |
❑ Yes ❑ No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
If YES, please answer the following: |
|
|
P |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
a.Was/Is your Social Security or SSI Disability application:
|
❑Approved? |
❑Denied? |
❑ Pending? |
❑ On Appeal? |
❑Unknown? |
|
|||||||
|
|
|
|||||||||||
b. |
Ifapprovedordenied,givethedateofthemostrecentdecisiononyourSocialSecurityorSSIdisability |
||||||||||||
|
application: |
|
|
|
|
L |
|
||||||
|
_________________________________________________________________________________ |
|
|||||||||||
c. |
Has your medical problem(s) worsened since the date in 5b above? |
|
Yes |
❑ No |
|
|
|
|
|||||
|
If YES, please explain: |
______________________________________________________________________ |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|||||||
|
_____________________________________________________________________________________________ |
|
|
||||||||||
d.Do you have any NEW medical problem(s) since the date in 5b, above, which you did NOT have when your Social Security or SSI disability decision was made?
❑ Yes ❑ No |
If YES, what medical problem(s)? _________________________________________ |
_____________________________________________________________________________________________ |
|
6. List all medical problems (physical, mental or emotional) that keep you from working or taking care of your personal needs. (Please attach additional sheet, if necessary.)
MEDICAL PROBLEM(S) |
E |
WHEN DID IT |
|
START (Month/Year) |
|||
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MC223 (05/07)
7. Have you received care in a clinic or hospital for your illness(es) or injury(ies) in the last |
|
COUNTY USE ONLY |
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
12 months? |
❑ Yes |
❑ No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
If YES, please fully answer the following: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of clinic/hospital |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
Patient/clinic or member number |
|
|
Clinic/hospital telephone number |
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of doctor(s) seen |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MC 220 Signed |
|
|
|
|
ADDRESS of clinic/hospital (number, street, suite) |
|
|
City |
|
|
|
|
|
State |
ZIP code |
|
|
❑ |
|
|
||||||||||||||||
|
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
Date first seen |
|
Date last seen |
|
|
|
|
|
|
|
Date of next appointment |
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Reason for the visit(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Did you stay in the hospital overnight? |
❑ Yes |
❑ No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
If YES, date(s) entered: |
|
_______________________________ date(s) left: ______________________________ |
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Were you seen in the emergency room? |
❑ Yes |
❑ No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
If YES, date(s) seen: |
_______________________________________________________________________________ |
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
List ALL medicines received: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
______________________________________________________________________ |
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
_____________________________________________________________________________________________________ |
|
|
|
|
|
|
||||||||||||||||||||||||
|
List ALL treatments received and the dates the treatments were received: |
_____________________ |
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
__________________________________________________________________________________________ |
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
||||||||||||||||||||||||||
8. List any additional clinic or hospital where you have been seen in the last 12 months. |
|
|
|
|
|
|
||||||||||||||||||||||||||
|
Name of clinic/hospital |
|
|
|
|
|
|
|
|
|
|
P |
|
|
|
|
|
|
|
|||||||||||||
|
Patient/clinic or member number |
|
|
Clinic/hospital telephone number |
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of doctor(s) seen |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MC 220 Signed |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❑ |
|||||||||||||||
|
ADDRESS of clinic/hospital (number, street, suite) |
|
|
City |
|
|
|
|
|
State |
ZIP code |
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date first seen |
|
|
|
|
|
|
|
Date last seen |
|
|
|
|
|
|
|
Date of next appointment |
|
|
|
|
|
|
|||||||||
|
Reason for the visit(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Did you stay in the hospital overnight? |
❑ Yes |
❑ No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
If YES, date(s) entered: |
_______________________________ date(s) left: ________________________________ |
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Were you seen in the emergency room? |
❑ Yes |
❑ No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
If YES, date(s) seen: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
_______________________________________________________________________________ |
|
|
|
|
|
|
|||||||||||||||||||||||||
|
List ALL medicines received: |
______________________________________________________________________ |
|
|
|
|
|
|
||||||||||||||||||||||||
|
_____________________________________________________________________________________________________ |
E |
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
List ALL treatments received and the dates the treatments were received: |
________________________ |
|
|
|
|
|
|
||||||||||||||||||||||||
|
_____________________________________________________________________________________________________ |
|
|
|
|
|
|
|||||||||||||||||||||||||
If you have been seen at additional clinics or hospitals in the last 12 months, complete page 8.
MC 223 (05/07)
Page 2 of 8
9. Have you been seen by any doctor outside of the clinic(s) or hospital(s) you have already |
COUNTY USE ONLY |
||
listed in the last 12 months? |
❑ Yes ❑ No |
|
|
|
|
||
|
|
|
|
If NO, go to number 10. If YES, please fully answer the following, if more than one doctor was seen please complete page 8 for all additional information:
Name of doctor(s)
|
Patient/clinic or member number |
|
Doctor’s telephone number |
|
|
|
|
||||
|
|
|
|
( |
) |
|
|
|
|
|
|
|
Address of doctor (number, street, suite) |
|
City |
|
STate |
ZIP code |
|
|
MC 220 Signed |
||
|
|
|
|
|
|
|
|
|
|
|
❑ |
|
Date first seen |
Date last seen |
|
|
Date of next appointment |
|
|
|
|||
|
Reason for theAvisit(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
List ALL medicines received: |
______________________________________________________________________ |
|
|
|
||||||
______________________________________________________________________________________________________ |
|
|
|
|
|||||||
|
List ALL treatments received and the dates the treatments were received: |
________________________ |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
||
|
______________________________________________________________________________________________________ |
|
|
|
|||||||
|
|
|
|
||||||||
10.Please list below if you have had any of the following tests in the last 12 months. Be sure to check yesornonexttoeachtest.(IFADDRESSOFDOCTOR,CLINIC,ORHOSPITALWASGIVEN ALREADY, LIST ONLY THE NAME AND DATE.)
TEST |
NAME AND ADDRESS OF OFFICE, CLINIC, |
DATE |
PERFORMED YES NO |
OR HOSPITAL WHERE TEST WAS COMPLETED |
(MO/YR) |
|
|
|
|
Name |
|
Electrocardiogram |
|
|
|
|
|
MC 220 Signed |
||
Address (number, street, suite) |
|
|
|
|||||
|
|
|
|
|
||||
(EKG) |
|
|
|
|
|
❑ |
||
|
|
City |
P |
State |
ZIP Code |
|
|
|
|
|
|
|
|||||
|
|
Name |
|
|
|
|
|
|
Treadmill |
|
|
|
|
MC 220 Signed |
|||
Address (number, street, suite) |
|
|
|
|||||
|
|
|
❑ |
|||||
(exercise heart test) |
|
|
|
|
|
|||
|
|
City |
|
State |
ZIP Code |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chest |
|
|
|
|
|
MC 220 Signed |
||
Address (number, street, suite) |
|
|
|
|||||
|
|
|
❑ |
|||||
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
City |
|
State |
ZIP Code |
|
|
|
|
|
|
|
|
||||
|
|
Name |
|
L |
|
|
|
|
Breathing Test |
|
|
MC 220 Signed |
|||||
Address (number, street, suite) |
|
|||||||
|
|
|
❑ |
|||||
(PFT) |
|
|
|
|
|
|||
|
|
|
|
|
|
|
||
|
|
City |
|
State |
ZIP Code |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Blood Tests |
|
|
|
|
|
MC 220 Signed |
||
Address (number, street, suite) |
|
|
|
❑ |
||||
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
City |
|
State |
ZIP Code |
|
|
|
|
|
|
|
|
||||
|
|
Name |
|
|
E |
|
|
|
Other |
|
|
|
MC 220 Signed |
||||
Address (number, street, suite) |
|
|
|
|||||
(Specify) |
|
|
|
|
|
❑ |
||
|
|
City |
|
State |
ZIP Code |
|
|
|
MC 223 (05/07)
Page 3 of 8
11. Have you had any other medical treatment or testing in the past 12 months? |
❑ Yes ❑ No |
COUNTY USE ONLY |
|
|
|
If NO, go to number 12.
If YES, complete page 8.
12.Is there anyone else (a friend, relative, social worker, rehab counselor, attorney, physical therapist, etc.) we may contact for information regarding your illness or injury and how it limits your daily activities or keeps you from working? ❑ Yes ❑ No
If YES, please list below:
Name |
A |
|
|
|
|
Address (number, street, suite) |
|
|
Telephone number |
Relationship to you |
|
()
Name
Address (number, street, suite)
Telephone number |
|
Relationship to you |
|
( |
) |
|
|
|
|
|
|
Name |
|
M |
|
|
|
||
Address (number, street, suite) |
|
|
|
|
|
|
|
Telephone number |
|
Relationship to you |
|
()
13.You may be asked to go to additional medical examinations to help evaluate your medical problem(s). (These examinations are free to you.)
Are you willing to go to additional medical examinations if needed? ❑ Yes ❑ No
PART
14.Describe your daily activities and tell us how much your condition limits your activities.
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
15.Describe your educational background.
a.Check the highest grade you finished in school:
❑ 1 ❑ 2 ❑ 3 ❑ 4 ❑ 5 ❑ 6 ❑ 7 ❑ 8 ❑ 9 ❑ 10 ❑ 11
❑ 12 or ❑ GED (same as finishing 12th grade) ❑ 12+
b.When finished? Month/year: ________________________________
c.Did you take special education classes? ❑ Yes ❑ No
16.Have you done any type of work for more than 30 days during the last 15 years? (This includes work done in another country.)
❑ Yes ❑ No
If NO, skip Part IV, go to Part V, page 7, for your signature.
If YES, answer Part IV, page 5, beginning with number 17.
MC 223 (05/07)
Page 4 of 8
|
|
|
|
|
|
PART |
|
|
|
|
COUNTY USE ONLY |
||
|
|
|
|
|
|
|
|
|
|||||
17. Describeallofthejobsyouhavedoneforatleast30daysduringthelast15years.Startwithyourmost |
|||||||||||||
recent job. (If you had more than two jobs, ask your county worker for additional pages.) |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. |
|
Job title |
|
|
|
Type of business |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dates worked (month/year) |
|
|
|
Hours per week |
Rate of pay |
Per hour/wk/mo |
|
|
|||
|
|
From: |
To: |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DESCRIPTION OF THE JOB (This is what I did and how I did it.)
These are the tools, machines, and equipment I used:
I took this long to learn the job: _______________ day(s) or _______________ month(s).
I wrote, completed reports, or performed similar duties: |
❑ Yes |
|
❑ No |
|
|
|
||||||
I had supervisory responsibilities: |
❑ Yes ❑ No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||
PHYSICAL ACTIVITY |
|
|
|
|
Circle One |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|||
I walked this many hours in an average workday: |
|
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
||
I stood this many hours in an average workday: |
|
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
||
I sat this many hours in an average workday: |
|
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
I climbed this much in an average workday:
❑ Never |
❑ Occasionally ❑ Frequently |
❑ Constantly |
|
|
|
I bent over this much in an average workday:
|
|
|
|
❑ Never |
❑ Occasionally ❑ Frequently |
❑ Constantly |
|
|
||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|||||
Heaviest weight I lifted: |
|
❑ 10 lbs |
❑ 20 lbs |
❑ 50 lbs |
❑ Over 100 lbs |
|
||||
I often lifted/carried up to: |
|
❑ 10 lbs |
❑ 20 lbs |
❑ 50 lbs |
❑ Over 100 lbs |
|
||||
|
|
|
|
|
|
|
||||
Did you have any of |
your current medical |
problem(s) |
when you |
performed this |
||||||
job? |
❑ Yes ❑ No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If NO, and you have had NO other jobs go to Part V, page 7, for your signature. If NO, but you have had other jobs, go to 17b, next page. If YES, please complete the following information.
Name of medical problem(s): ___________________________________________________________
Did your employer make special arrangements (such as extra breaks, special equipment, change in job duties, etc.) so you could continue to work? ❑ Yes ❑ No
If YES, describe the special arrangements made: ________________________________________
Did you have to stop working because of your medical problem(s)? ❑ Yes ❑ No
If YES, when? Month ____________________________________ Day _________ Year _________
Have you done any other work for more than 30 days during the last 15 years? ❑Yes ❑No If NO, go to Part V, page 7 for your signature. If YES, continue on 17b, next page.
MC 223 (05/07)
Page 5 of 8
17. b. |
|
Job title |
|
|
|
Type of business |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dates worked (month/year) |
|
|
|
Hours per week |
Rate of pay |
Per hour/wk/mo |
|
||
|
|
From: |
To: |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
DESCRIPTION OF THE JOB (This is what I did and how I did it.)
These are the tools, machines, and equipment I used:
I took this long to learn the job: _______________ day(s) or _______________ month(s).
I wrote, completed reports, or performed similar duties: |
|
|
|
Yes |
|
|
No |
|
|
|
|
|
||||||||
I had supervisory responsibilities: |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
PHYSICAL ACTIVITY |
|
|
|
|
|
|
|
|
Circle One |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
I walked this many hours in an average workday: |
|
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
|
|
||||||||
I stood this many hours in an average workday: |
|
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
|
|
||||||||
I sat this many hours in an average workday: |
|
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
I climbed this much in an average workday: |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Never |
|
|
Occasionally |
|
Frequently |
|
|
Constantly |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
I bent over this much in an average workday: |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Never |
|
|
Occasionally |
|
Frequently |
|
|
Constantly |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Heaviest weight I lifted: |
|
|
10 lbs |
|
|
20 lbs |
|
50 lbs |
|
|
Over 100 lbs |
|||||||||
I often lifted/carried up to: |
|
|
10 lbs |
|
|
20 lbs |
|
50 lbs |
|
|
Over 100 lbs |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Did you have any of your current medical problem(s) when you performed this job?  Yes
Yes  No
No
If NO, and you have had NO other jobs go to Part V, page 7, for your signature. If NO, but you have had other jobs, ask your county worker for additional pages. If YES, please complete the following information.
Name of medical problem(s): ___________________________________________________________
Did your employer make special arrangements (such as extra breaks, special equipment, change
in job duties, etc.) so you could continue to work?  Yes
Yes  No
No
If YES, describe the special arrangements made: ________________________________________
Did you have to stop working because of your medical problem(s)? |
|
Yes |
No |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
If YES, when? Month |
____________________________________ |
Day |
_________ |
|
Year |
________ |
|
|||
Have you done any other work for more than 30 days during the last 15 years? |
|
|
|
|
|
|||||
|
|
|
|
|
||||||
Yes |
No |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
If NO, go to Part V, page 7 for your signature. If YES, ask your county worker for additional pages to complete.
COUNTY USE ONLY
MC 223 (05/07)
Page 6 of 8
PART
I declare under penalty of perjury under the laws of the United States of America and the State of California that the information contained in this Supplemental Statement of Facts is true and correct.
Signature of Applicant |
Date |
➧ |
|
|
|
Signature of Witness (If applicant signed with a mark) |
Date |
➧ |
|
|
|
Signature of person helping applicant fill out the form |
Date |
➧ |
|
You will need to sign an authorization for release of information for each clinic, hospital, and testing facility that you list and for each doctor you saw outside of a clinic or hospital. Your county worker will provide you with additional forms which you will need to sign.
MC 223 (05/07)
Page 7 of 8
Continued answer(s) to question(s) number 8 on page 2, number 9 on page 3, and number 10 on page |
COUNTY USE ONLY |
|
3. If you need more room, please ask your county worker for additional pages to complete. |
||
|
||
List any additional clinic or hospital where you have been seen in the last 12 months: |
|
Name of clinic/hospital
Patient/clinic or member number |
Clinic/hospital telephone number |
|
|
( |
) |
Name of doctor(s) seen |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
A |
|
|
|
|
|
City |
|
|
State |
ZIP code |
|
||||||
ADDRESS of clinic/hospital (number, street, suite) |
|
|
|
MC 220 Signed |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❑ |
Date first seen |
|
Date last seen |
|
|
|
|
|
Date of next appointment |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Reason for the visit(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||||||
Did you stay in the hospital overnight? |
❑ Yes |
❑ No |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
If YES, date(s) entered: |
______________________________ |
date(s) left: |
__________________________________ |
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Were you seen in the emergency room? |
❑ Yes |
❑ No |
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If YES, date(s) seen: |
________________________________________________________________________ |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
List ALL medicines received: |
_______________________________________________________________________ |
|
|
||||||||||||||
______________________________________________________________________________________________________ |
|
|
|||||||||||||||
List ALL treatments received and the dates the treatments were received: |
________________________ |
|
|
||||||||||||||
______________________________________________________________________________________________________ |
|
|
|||||||||||||||
List any additional doctor you saw outside of the clinic(s) or hospital(s) you have already listed:
Name of doctor(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient/clinic or member number |
|
|
P |
Doctor’s telephone number |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|||||
|
|
|
|
( |
) |
|
|
|
|
|
|
|
Name of doctor(s) seen |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
ADDRESS of doctor (number, street, suite) |
City |
|
State |
ZIP code |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||
Date first seen |
|
Date last seen |
|
|
|
Date of next appointment |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MC 220 Signed |
Reason for the visit(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❑ |
|
|
|
|
|
|
|
|
|
|
|
|
|
List ALL medicines received: |
|
|
|
|
|
|
|
|
|
________________________________________________________________ |
|
|
|
|
|
|
|
|
|
||||||
______________________________________________________________________________________________________ |
|
|
|
|||||||||
|
|
|
||||||||||
List ALL treatments received and the dates the treatments were received: |
________________________ |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
______________________________________________________________________________________________________ |
|
|
|
|||||||||
List any additional tests you have had in the last 12 months:
|
|
NAME AND ADDRESS OF OFFICE, CLINIC, OR HOSPITAL |
|
DATE |
|
||||
|
TEST PERFORMED |
|
WHERE TEST(S) WAS COMPLETED. |
|
|
(MO/YR) |
|
||
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address (number, street, suite) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
State |
ZIP code |
E |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
MC 220 Signed |
|
||||
|
|
Name |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
❑ |
|
|
|
Address (number, street, suite) |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MC 220 Signed |
|
|
|
City |
State |
ZIP code |
|
|
|
|
|
|
|
|
|
|
❑ |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MC 223 (05/07)
Page 8 of 8
Form Data
| Fact Name | Description |
|---|---|
| Governing Law(s) | The form is governed by California state law under the Department of Health Care Services. |
| Purpose of the Form | It serves as an Applicant’s Supplemental Statement of Facts for Medi-Cal, assisting in the evaluation for eligibility. |
| Content Overview | Includes personal information, medical information, social and educational information, and work history to assess Medi-Cal eligibility and needs. |
| Sections Requiring Detailed Medical Information | Applicants must detail their medical conditions, treatments, hospital visits, and any Social Security Disability or Supplemental Security Income (SSI) Disability benefits applied for or received. |
Instructions on Utilizing Mc 223
Filling out the MC 223 form is an important process for those seeking to provide comprehensive details about their personal, medical, social, and educational information. This guide outlines the structured steps needed to accurately complete the form, ensuring that all necessary information is communicated effectively.
- Start with PART I—PERSONAL INFORMATION. Fill in your full name, Social Security number, date of birth, any other names used, your sex, height, and weight.
- Enter your home address, including city, state, and ZIP code. If your mailing address differs, provide that information as well.
- Provide a daytime telephone number and indicate the best time for contact. If you have no phone or prefer messages to be left at a different number, mark the appropriate box.
- Answer whether you speak English and if you require an interpreter. If you do need an interpreter, supply the interpreter’s name and phone number. Indicate the language you speak if English is not your preference.
- Move to PART II—MEDICAL INFORMATION. Indicate if you have applied for Social Security Disability or Supplemental Security Income (SSI) in the past two years. If affirmative, provide details as requested about the application’s status, any recent decisions, and whether your medical condition has worsened or new medical problems have arisen since your last application.
- List all medical problems that prevent you from working or taking care of personal needs. Attach additional sheets if necessary.
- Detail any clinic or hospital care received in the last 12 months, including the clinic's or hospital's name, addresses, doctors seen, dates of visits, reasons for visits, any overnight stays or emergency room visits, medications received, and treatments undergone.
- If applicable, list any additional clinics or hospitals where you have been seen in the last 12 months.
- Include information about any doctors seen outside of the listed clinics or hospitals in the last 12 months.
- Check off and provide details for tests such as electrocardiograms, treadmill tests, chest X-rays, breathing tests, blood tests, and any others conducted in the last year.
- Answer whether you have had any other medical treatment or testing in the past 12 months. If so, additional details should be provided on page 8 of the form.
- Indicate if there is someone who can provide additional information about your illness or injury. Provide their name, address, telephone number, and relationship to you.
- Confirm willingness to attend additional medical examinations if necessary.
- Proceed to PART III—SOCIAL AND EDUCATIONAL INFORMATION. Describe your daily activities, limitations due to your condition, highest grade completed, educational background, and whether you attended special education classes.
- Discuss your work history in PART IV, starting with the most recent job. Include job title, type of business, dates worked, hours per week, rate of pay, and detailed descriptions of the job duties and physical activities required. If you’ve had more than two jobs within the last 15 years, ask for additional pages to provide complete employment history.
- Finally, sign and date the form on page 7, indicating the completion of the MC 223 form.
After submitting the MC 223 form, your information will be reviewed by the relevant department. This process is crucial for accurately assessing your needs and eligibility for services. Expect to be contacted for any additional information or clarification needed, or to arrange further medical evaluations as part of the assessment process.
Obtain Answers on Mc 223
-
What is the purpose of the MC 223 form?
The MC 223 form is used by applicants to provide supplementary information required for Medi-Cal eligibility determination in California. It collects personal, medical, social, educational, and work history information to support an applicant's claim for health benefits.
-
Who needs to fill out the MC 223 form?
Individuals applying for Medi-Cal benefits in California who have been requested by their county’s health and human services agency to provide additional information about their medical condition, work history, and personal circumstances should complete the form.
-
What information do I need to provide in Part I of the MC 223 form?
Part I requires personal information such as your name, date of birth, social security number, sex, height, weight, contact information, and whether you need an interpreter, along with the languages you speak.
-
What information is required in Part II regarding medical information?
In Part II, you must detail your Social Security Disability or Supplemental Security Income (SSI) Disability benefits application status, list all medical conditions, detail any recent hospital or clinic care, list any doctors seen outside of clinics or hospitals, and note any tests you have undergone in the past 12 months.
-
Can I add additional pages if there is not enough space on the form?
Yes, if you need more space to provide a comprehensive list of medical problems, treatments, clinic or hospital visits, or any other requested information, you are encouraged to attach additional sheets.
-
How do I complete Part III regarding social and educational information?
In Part III, you should describe your day-to-day activities, any limitations due to your condition, your highest grade completed or educational qualifications like a GED, and whether you attended special education classes.
-
What work history information is necessary for Part IV?
Part IV asks for a detailed description of jobs you’ve done in the last 15 years, including job titles, types of business, dates worked, hours per week, pay rate, physical activities involved, and whether your medical condition affected your work ability.
-
What should I do if I need an interpreter to help fill out the MC 223 form?
If you require an interpreter, you should indicate this need in Part I, section 4b of the form, including the interpreter's name and contact information, along with the best time to call them.
-
Where do I submit the completed MC 223 form?
The completed MC 223 form should be submitted to your local county health and human services agency. It’s important to check with your county office for specific submission guidelines, whether by mail, in person, or electronically, if available.
Common mistakes
Filling out the Mc 223 form, an essential document for Medi-Cal applicants in California, can sometimes feel like navigating through a maze without a map. Individuals often stumble over the same roadblocks, making errors that can delay or even derail their application process. Let's shine a light on four common mistakes people make when filling out this form and how avoiding them can make the journey smoother.
- Incomplete Personal Information
Part I of the MC 223 form requests personal details such as name, Social Security number, and contact information. A frequent hiccup occurs when applicants leave fields blank or provide incomplete information. Ensuring every question is answered fully can prevent unnecessary delays in the process.
- Omission of Medical Details
In Part II, the form dives into medical information, inquiring about conditions that affect the applicant's ability to work or perform daily activities. Skipping questions or not providing sufficient detail about medical conditions and treatments is a common slip-up. It's crucial to list all relevant medical problems, treatments, and hospital visits to give a comprehensive view of one's health status.
- Failure to Include Additional Sheets
Space on the MC 223 form is limited. When applicants have more information than the form can accommodate, such as an extensive medical history, they should attach additional sheets. However, some forget to do so or don't realize it's an option. Attaching extra pages with complete information ensures the review team has all they need to assess the application accurately.
- Incorrect or Outdated Information
Providing information that is either incorrect or outdated, especially regarding contact details for clinics, hospitals, or doctors seen in the last 12 months, is another common mistake. It's imperative to double-check that all information is current and accurate to avoid any communication issues between Medi-Cal representatives and medical providers.
Avoiding these pitfalls when filling out the MC 223 form isn't just about preventing delays; it's about ensuring that the assessment of one's need for medical assistance through Medi-Cal is as accurate and swift as possible. A careful review of the form before submission can make a significant difference in the application process.
Documents used along the form
Understanding the complete scope of documentation required for comprehensive medical and disability assessments, such as those initiated with the MC 223 form, is crucial. This form, utilized within the California Health and Human Services Agency, Department of Health Care Services, is just the starting point for applicants seeking Medi-Cal benefits due to disability or health-related issues. Accompanying documents play a pivotal role in providing a full picture of an applicant’s condition and needs. Here is a list of eight other forms and documents commonly used alongside the MC 223 form:
- MC 220 Form: This document is a medical certification form used by doctors to report a patient's health status and the medical necessity for Medi-Cal benefits. It complements the MC 223 by providing professional verification of the conditions listed by the applicant.
- Social Security Disability Benefits Application: Many individuals applying for Medi-Cal due to a disability will also apply for Social Security Disability Insurance (SSDI) or Supplemental Security Income (SSI). Proof of application or receipt of these benefits can be crucial in the Medi-Cal application process.
- Proof of Income: Documents demonstrating the applicant's income, such as pay stubs, tax returns, or benefit statements, are necessary to establish financial eligibility for Medi-Cal.
- Proof of California Residency: Documents like utility bills, rental agreements, or California ID cards establish residency, a requirement for Medi-Cal eligibility.
- Medical Records: Comprehensive medical records provide evidence of an applicant's medical conditions and previous treatments, supporting the information provided in the MC 223 form.
- Prescription Medication Records: Lists of current and past medications can demonstrate the ongoing and historical needs of the applicant, substantiating the claims of medical necessity.
- Authorization for Release of Information: This form allows the California Department of Health Care Services and other relevant entities to obtain and share medical and financial information pertinent to the Medi-Cal application.
- Appeal Documentation: If the applicant has previously applied and been denied Medi-Cal benefits or disability benefits from Social Security, documentation related to the appeal process can be relevant, especially if circumstances have changed.
Together, these documents form a comprehensive dossier that supports an individual’s application for Medi-Cal benefits, highlighting their health status, financial situation, and the specific reasons they require assistance. It's a holistic approach that ensures the Department of Health Care Services has all necessary information to make an informed decision regarding eligibility and the level of support required. Understanding the importance and role of each document can significantly streamline the application process for applicants and their families, leading towards a more straightforward path to receiving essential health care benefits.
Similar forms
The SSA-3368 form (Disability Report - Adult) used by the Social Security Administration is similar to the MC 223 form. Just like the MC 223 form, it gathers personal and medical information to support an individual's disability claim, including the nature of their disability, their work history, and treatments or tests they have undergone.
The I-485 form (Application to Register Permanent Residence or Adjust Status) issued by U.S. Citizenship and Immigration Services shares characteristics with the MC 223 form. Both require detailed personal information, including past addresses, employment history, and specific demographic information, to process the application accurately.
The VA Form 21-526EZ (Application for Disability Compensation and Related Compensation Benefits) used by the Department of Veterans Affairs resembles the MC 223 form in the way it collects detailed medical and personal information to assess the eligibility for disability benefits.
The DS-260 (Immigrant Visa Electronic Application), also requires comprehensive personal, familial, and medical information, similar to the information requested in the MC 223 form, as part of the process for individuals seeking an immigrant visa to the United States.
The Medical Examination Report Form for Commercial Driver License (CDL), which is required for commercial drivers, shares similarities with the MC 223 by requiring medical history information, tests performed, and details about physical health that could affect the applicant's ability to perform job duties.
The Form I-693 (Report of Medical Examination and Vaccination Record) used in conjunction with certain immigration processes gathers detailed medical information, including a history of vaccinations and results from medical examinations, paralleling the detailed health information required on the MC 223 form.
FL-150 (Income and Expense Declaration) used in family law courts in California, while focused on financial information, requires detailed personal income, expense, and employment information, akin to the work history and financial capacity aspects covered in the MC 223 form.
The WIC Program Application, which assists women, infants, and children, requires detailed information about the health and nutrition status of applicants, drawing parallels to the medical history and present health condition details required by the MC 223 form.
The FAFSA (Free Application for Federal Student Aid), used by students to apply for financial aid, although primarily focused on financial information, requires detailed personal and demographic information. It aims to assess the applicant's eligibility for aid, similar to the eligibility assessment objectives of the MC 223 form.
HUD-1 Settlement Statement, used in real estate transactions, though focusing on financial exchanges, requires detailed identification of all parties involved in the transaction, mirroring the requirement for detailed personal information found on the MC 223 form.
Dos and Don'ts
When you're filling out the MC 223 form for Medi-Cal, it is crucial to approach it carefully to avoid common mistakes. Here are some do's and don'ts that can guide you through the process:
- Do review the entire form before you start filling it out to understand what information you will need to provide.
- Do gather all necessary documents, such as medical records, social security information, and proof of income, before you begin. This ensures the information you provide is accurate and consistent.
- Do use a black or blue ink pen if you are filling out a paper copy of the form. This makes your responses legible and photocopy-friendly.
- Do be as specific as you can when listing your medical conditions, treatments received, and how they affect your daily life. Vague answers can lead to processing delays.
- Do double-check the completeness and accuracy of your answers before submitting the form to minimize the chances of it being returned for corrections.
- Don’t leave any sections blank unless instructed. If a question does not apply to you, it's safer to fill it with “N/A” (Not Applicable) than to leave it empty.
- Don’t guess information. If you’re unsure about specific details, such as exact dates or dosages, make the effort to verify them before filling them out. Incorrect information may lead to unnecessary complications.
- Don’t use correction fluid or tape on the form. If you need to make corrections, draw a single line through the mistake, write the correct information nearby, and initial the change if there’s space. This keeps the form tidy and your information clear.
- Don’t forget to sign and date the form. An unsigned application is considered incomplete and will not be processed.
Adhering to these guidelines will help ensure your application is complete and properly reviewed, making the process smoother and hopefully faster for both you and the processing agency.
Misconceptions
When it comes to the MC 223 form, commonly used in the process of applying for Medi-Cal benefits in California, there are several misconceptions that tend to circulate. Understanding the form correctly is crucial to ensuring applications are filled out accurately and benefits can be processed efficiently. Here are six common misconceptions and the reality of each:
- The form is only for individuals with a disability. While Part II of the MC 223 form focuses on medical information, including disability, the form itself is not solely for those with disabilities. It's a comprehensive document that gathers various kinds of information from applicants, including personal, social, and educational details, to assess their eligibility for Medi-Cal.
- You must have Social Security Disability to apply. Question 5 inquires if you've applied for Social Security Disability or Supplemental Security Income (SSI) Disability benefits in the last two years. However, this does not mean that having applied or been approved for these benefits is a prerequisite for Medi-Cal. It's a question aimed at gathering more information about your situation.
- Only physical health problems are relevant. The MC 223 form requests information about all medical problems affecting your ability to work or take care of yourself, including physical, mental, or emotional issues. It's important to disclose all relevant health problems, not just physical ones.
- The form doesn't consider language barriers. The form explicitly asks if you speak English and if you have an interpreter, indicating that it's designed to accommodate non-English speakers and consider language barriers in the application process.
- If you haven’t been hospitalized, you should skip good portions of the form. While sections 7 and 8 ask about clinic or hospital visits, it's essential to fill out every part of the form applicable to your situation, including detailing any doctor visits outside hospitals that have contributed to understanding your health status. Skipping sections without reviewing them might lead to omitting important information.
- Only recent medical information is necessary. Although the form asks for recent hospital visits, doctor visits, and tests, it's vital to provide a comprehensive medical history that covers the required time frames specified in the form. For instance, question 9 asks about doctor visits outside of listed clinics or hospitals in the last 12 months, indicating the need for both recent and slightly older medical information.
Correctly understanding and filling out the MC 223 form is a key step in applying for Medi-Cal. Clearing up these misconceptions ensures that applicants provide thorough and accurate information, which can help streamline the processing of their application. Always refer to the instructions on the form and seek assistance if you're unsure how to answer specific questions.
Key takeaways
Here are key takeaways for filling out and using the MC 223 form, also known as the Applicant's Supplemental Statement of Facts for Medi-Cal:
- Ensure all personal information is accurately entered in Part I, including your name, Social Security number, date of birth, and contact details.
- If you do not speak English or prefer another language for communication, specify this in question 4a and 4b, providing the details of an interpreter if needed.
- Disclose any applications for Social Security Disability or Supplemental Security Income (SSI) Disability benefits within the last two years in Part II.
- List all medical conditions that affect your ability to work or manage personal care, and provide details about any hospital or clinic care received in the past 12 months.
- Include comprehensive information about any medical tests performed in the last 12 months, specifying the type of test, where it was performed, and the date.
- If you have seen additional doctors or received further medical treatment not already listed, provide their details and the reasons for the visits.
- Indicate if there is someone (a friend, relative, or professional) who can provide additional information about your condition and its impact on your daily activities.
- Be ready to participate in additional medical examinations if required, to further evaluate your medical conditions.
- For the social and educational information section, describe how your condition limits your daily activities and your educational background.
- Detail your work history for the last 15 years in Part IV, highlighting job responsibilities, physical activities involved, and accommodations made for medical conditions.
Remember, providing detailed and accurate information on the MC 223 form is crucial for Medi-Cal to assess your eligibility and needs properly. If additional space is needed for any answers, attach extra sheets as necessary.
Popular PDF Forms
Connecticut 7B - Fulfill your legal duty to show workers’ compensation insurance with ease using the Connecticut 7B form as a construction project leader.
Dd Form 2708 - An essential part of the legal documentation surrounding the transfer of custody, capturing key data points including recipient credentials and detainee information.
Lien Release Statement - The owner information section collects details about the vehicle's owner at the time of the lien agreement.