Blank Memorial Hermann Release PDF Template
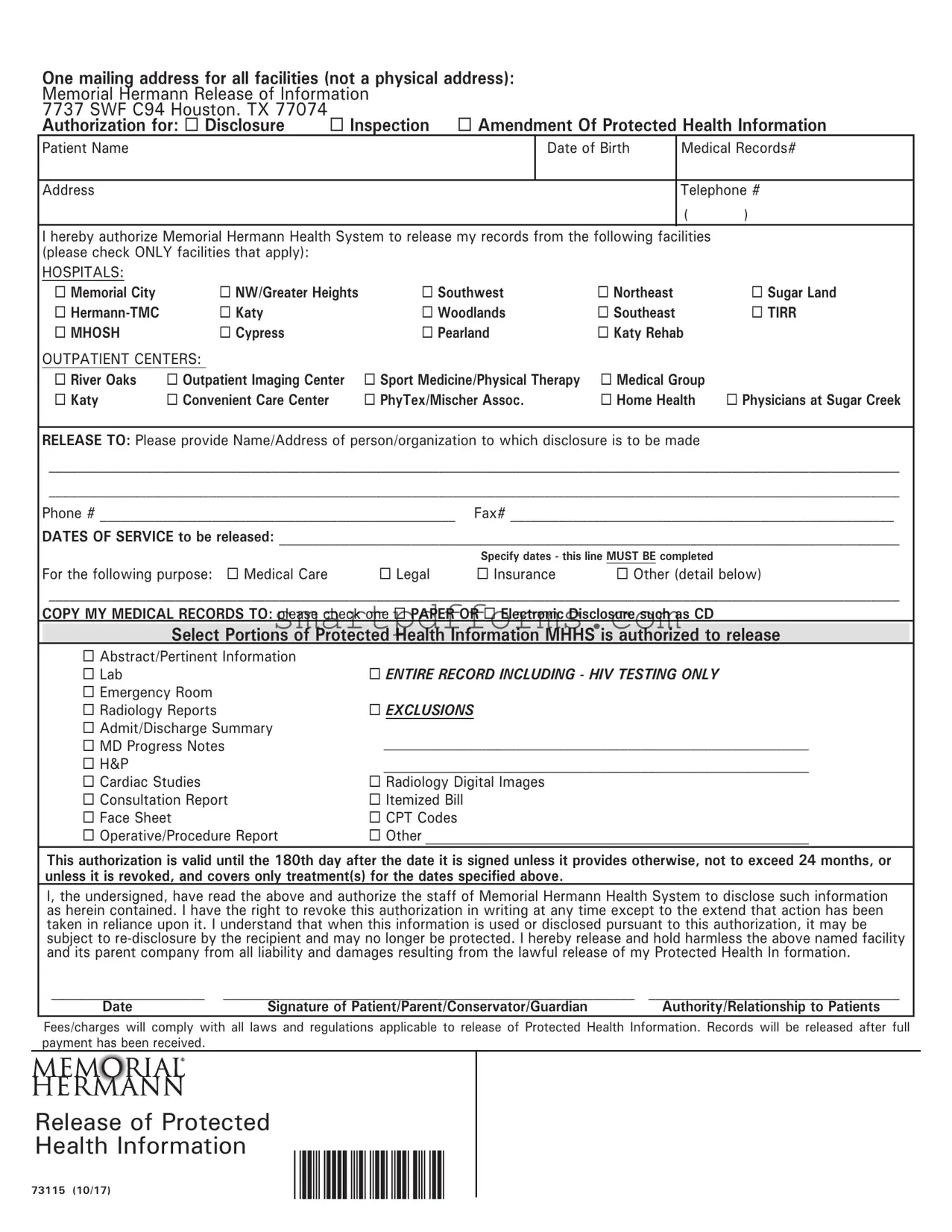
In the realm of healthcare, the protection and authorization of personal medical information are paramount. The Memorial Hermann Release Form embodies this principle by providing a structured method for patients to permit the disclosure of their health records. This document enables the comprehensive management of Protected Health Information (PHI) across various facilities affiliated with the Memorial Hermann Health System. Designed to facilitate an organized process, the form addresses the release of information for reasons ranging from medical care to legal and insurance purposes. Patients specify which facilities' records to disclose, the type of information needed—be it an abstract of pertinent information, lab results, the entire record, or specific elements like emergency room reports and radiology digital images—and the format in which to receive this information, such as paper or electronic media. With its provision for specifying the recipient of the disclosed information and the precise service dates of the records requested, the form ensures a targeted approach to information sharing. It also outlines the validity period of the authorization, the rights of patients to revoke this permission, and the applicable fees in compliance with laws governing the release of PHI. The Memorial Hermann Release Form thus stands as a critical tool, ensuring that the dissemination of health information is handled with the utmost respect for privacy and legal obligations, while empowering patients in their healthcare management.
Preview - Memorial Hermann Release Form
One mailing address for all facilities (not a physical address): |
|
|
|
||||
Memorial Hermann Release of Information |
|
|
|
||||
7737 SWF C94 Houston. TX 77074 |
Inspection Amendment Of Protected Health Information |
||||||
Authorization for: Disclosure |
|||||||
Patient Name |
|
|
|
Date of Birth |
Medical Records# |
||
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
Telephone # |
|
|
|
|
|
|
|
( |
) |
I hereby authorize Memorial Hermann Health System to release my records from the following facilities |
|
||||||
(please check ONLY facilities that apply): |
|
|
|
|
|
|
|
HOSPITALS: |
|
|
|
|
|
|
|
Memorial City |
NW/Greater Heights |
Southwest |
Northeast |
|
Sugar Land |
||
|
Katy |
|
Woodlands |
Southeast |
|
TIRR |
|
MHOSH |
Cypress |
|
Pearland |
Katy Rehab |
|
||
OUTPATIENT CENTERS: |
|
|
|
|
|
|
|
River Oaks |
Outpatient Imaging Center |
Sport Medicine/Physical Therapy |
Medical Group |
|
|||
Katy |
Convenient Care Center |
|
PhyTex/Mischer Assoc. |
Home Health |
Physicians at Sugar Creek |
||
RELEASE TO: Please provide Name/Address of person/organization to which disclosure is to be made
__________________________________________________________________________________________________________________________
__________________________________________________________________________________________________________________________
Phone # ___________________________________________________ Fax# _______________________________________________________
DATES OF SERVICE to be released: _________________________________________________________________________________________
|
|
Specify dates - this line MUST BE completed |
|
For the following purpose: Medical Care |
Legal |
Insurance |
Other (detail below) |
__________________________________________________________________________________________________________________________
COPY MY MEDICAL RECORDS TO: please check one PAPER OR Electronic Disclosure such as CD
Select Portions of Protected Health Information MHHS is authorized to release
Abstract/Pertinent Information |
|
Lab |
ENTIRE RECORD INCLUDING - HIV TESTING ONLY |
Emergency Room |
|
Radiology Reports |
EXCLUSIONS |
Admit/Discharge Summary |
_____________________________________________________________ |
MD Progress Notes |
|
H&P |
_____________________________________________________________ |
Cardiac Studies |
Radiology Digital Images |
Consultation Report |
Itemized Bill |
Face Sheet |
CPT Codes |
Operative/Procedure Report |
Other _______________________________________________________ |
This authorization is valid until the 180th day after the date it is signed unless it provides otherwise, not to exceed 24 months, or
unless it is revoked, and covers only treatment(s) for the dates specified above.
I, the undersigned, have read the above and authorize the staff of Memorial Hermann Health System to disclose such information as herein contained. I have the right to revoke this authorization in writing at any time except to the extend that action has been taken in reliance upon it. I understand that when this information is used or disclosed pursuant to this authorization, it may be subject to
______________________ |
___________________________________________________________ |
____________________________________ |
Date |
Signature of Patient/Parent/Conservator/Guardian |
Authority/Relationship to Patients |
Fees/charges will comply with all laws and regulations applicable to release of Protected Health Information. Records will be released after full payment has been received.
Release of Protected
Health Information
73115 (10/17)
Form Data
| Fact Number | Description |
|---|---|
| 1 | The form includes one mailing address for all facilities, located in Houston, TX. |
| 2 | Authorization options include Disclosure, Inspection, and Amendment of Protected Health Information. |
| 3 | Patients can authorize the release of records from specific Memorial Hermann facilities by selecting them on the form. |
| 4 | Designated recipients for the disclosed information must be specified, including their name, address, phone number, and fax number. |
| 5 | Records can be requested in paper form or electronic form, such as on a CD. |
| 6 | This authorization form is valid until the 180th day after signing, but not exceeding 24 months, unless revoked earlier. |
| 7 | Fees for processing the release of information are compliant with all applicable laws and regulations. |
Instructions on Utilizing Memorial Hermann Release
Filling out the Memorial Hermann Release form is a critical step in the process of authorizing the disclosure of your protected health information for various purposes like medical care, legal matters, insurance, and more. This process ensures that your medical records are shared securely and with your consent, according to your specified preferences. To complete the form accurately, it's important to follow each step carefully to ensure that all necessary information is provided so that your request can be processed efficiently without any delays.
- Find the "Patient Name" section and enter your full name as it appears in your medical records.
- Next to your name, fill in your "Date of Birth" in the specified format.
- Enter your "Medical Records#" if known; otherwise, proceed to the next step.
- Under "Address," provide your current home address where correspondence can be sent if necessary.
- Fill in your "Telephone #" with the best number to reach you, including the area code.
- Review the list of facilities under "HOSPITALS" and "OUTPATIENT CENTERS." Check ONLY the boxes next to the facilities from which you are authorizing the release of your records.
- In the "RELEASE TO" section, write the full name and address of the person or organization to whom the information is to be disclosed, followed by their phone and fax numbers.
- Specify the "DATES OF SERVICE to be released" by indicating the range of dates for which your medical records are needed. This line must be completed for the request to be processed.
- Select the purpose of the release by checking the appropriate box: "Medical Care," "Legal," "Insurance," or specify another purpose under "Other."
- Choose the format in which you'd like your medical records to be copied by selecting either "PAPER" or "Electronic Disclosure such as CD."
- Identify which portions of your Protected Health Information you authorize to release by checking the appropriate boxes. If you want the "ENTIRE RECORD," ensure to only select that option if it applies. Note any exceptions in the provided space.
- Read the statement at the bottom of the form which outlines the validity of the authorization, your rights, and other legal information. Ensure you fully understand this before proceeding.
- Sign and date the form in the spaces provided at the bottom. If you are not the patient, specify your "Authority/Relationship to Patient."
- Review the form for accuracy and completeness before submitting it to the address provided at the top, ensuring full compliance with any fees or charges as noted.
Once the form has been correctly filled out and submitted, the authorized personnel at Memorial Hermann Health System will process your request. The release of information will be executed as per your directions on the form, allowing the specified recipients to access or receive your medical records for the stated purposes. It is crucial to follow up if you do not receive an acknowledgment of your request within a reasonable timeframe, to ensure your information is being processed as expected.
Obtain Answers on Memorial Hermann Release
-
What is the purpose of the Memorial Hermann Release form?
This form serves as an authorization for Memorial Hermann Health System to release a patient's records to specified individuals or organizations. It is used when a patient needs to make their health information available to other parties, such as for medical care, legal issues, insurance purposes, or other specified reasons. The form ensures the patient's consent is obtained before any protected health information (PHI) is disclosed.
-
How can I specify which records or portions of my health information I want to be released?
On the form, you have the option to select specific types of information that you agree to disclose, such as lab results, HIV testing, radiology reports, and more. You can choose to release the entire record, only pertinent abstractions, or specific parts of your medical history by checking the appropriate boxes provided. It's important to clearly mark your choices to ensure only the selected portions of your PHI are shared.
-
Can I choose the format in which my medical records are released?
Yes, the form allows you to indicate your preference for the format in which your medical records should be disclosed. You can select either paper copies or electronic disclosure, such as a CD. This choice ensures that the records are delivered in a format that is most convenient and accessible for your needs or for the receiving party's requirements.
-
How long is the authorization I give on the Memorial Hermann Release form valid?
The authorization is valid until the 180th day after it is signed, not to exceed 24 months, unless otherwise stated on the form. However, you retain the right to revoke this authorization at any time in writing. Once revoked, the form will no longer hold, except in the case where actions have already been taken based on the initial consent.
-
Is there a fee associated with the release of my medical records?
Yes, there may be a fee for the provision of your medical records, which complies with all applicable laws and regulations concerning the release of Protected Health Information. Records will be released after full payment of these fees. The form or accompanying documentation should provide specific details about these charges or how to inquire about them.
-
What if I need to revoke the authorization I granted on the Memorial Hermann Release form?
You have the right to revoke the authorization you have given at any time. To do so, you must submit your revocation in writing. However, it is important to note that the revocation cannot affect any disclosures that have already taken place in reliance on your initial consent. Ensuring you promptly communicate your revocation is crucial to stopping further sharing of your health information.
Common mistakes
-
One common mistake is neglecting to specify the exact facilities from which records should be released. The form provides a checklist of hospitals and outpatient centers, requiring the requester to check only those that apply. Failing to check the appropriate facilities can lead to incomplete information being released or the request being denied for lack of clarity.
-
Omitting the dates of service needed is another error that can significantly delay the processing of the form. The line that mandates specifying dates must be completed to ensure that the right records, corresponding to the correct periods of care, are released. This detail is crucial for the purpose it’s being requested for, whether for medical care, legal matters, insurance, or other reasons.
-
Choosing between paper or electronic disclosure is a decision some fail to make when filling out the form. This choice determines how the receiving party will get the records. Not making a selection can result in delays or the records being sent in a format that might not be useful to the recipient.
-
Finally, a mistake often made by individuals is not signing and dating the authorization form, which is a critical step for the form to be valid. The absence of a signature and date makes the request invalid, as it lacks the necessary consent to release the protected health information. Additionally, it's vital to ensure that the individual signing the form has the authority to do so, whether they are the patient, parent, conservator, or guardian.
Documents used along the form
When managing healthcare information, particularly in engaging with forms like the Memorial Hermann Release form, understanding the ecosystem of related documents is crucial. These documents play significant roles in ensuring the seamless transfer, protection, and utilization of health information for various purposes such as medical care, legal proceedings, and insurance claims. Below is a list that illuminates some of these essential forms and documents that often accompany or are utilized in conjunction with the Memorial Hermann Release form.
- Consent for Treatment Form: This form is foundational in healthcare, giving medical professionals permission to administer treatment. It's often required before any medical procedure can occur, ensuring that the patient or their legal guardian understands the nature of the treatment and the associated risks.
- Notice of Privacy Practices: This document informs patients about how their health information may be used and disclosed by the healthcare provider. It also outlines the patients' rights regarding their health information, according to the Health Insurance Portability and Accountability Act (HIPAA).
- Advance Directive Form: An advance directive is crucial for future healthcare decisions. It outlines a patient's wishes regarding medical treatment in scenarios where they're unable to communicate their decisions due to illness or incapacity.
- Authorization for Use and Disclosure of PHI: This form is more specific than the Memorial Hermann Release form in that it pertains to the use and disclosure of Protected Health Information (PHI) for reasons outside the standard healthcare operations, payments, and treatments.
- Request for Amendment of Health Record: Patients who believe that their health records contain errors can use this form to request an amendment or correction. It is an essential right under HIPAA, ensuring that information is accurate and up-to-date.
- Health Insurance Portability and Accountability Act (HIPAA) Authorization Form: Similar to the Memorial Hermann Release form, the HIPAA authorization form is a legal document that allows healthcare providers to use or disclose an individual's health information for purposes beyond treatment, payment, or healthcare operations.
- Medical Power of Attorney Form: This legal document allows an individual to appoint someone they trust to make healthcare decisions on their behalf if they become unable to make such decisions for themselves.
- Proof of Representation Form: This form is necessary when a person is acting on behalf of the patient in legal or healthcare matters. It provides the medical facility with proof that the individual has the authority to access the patient's health information or make decisions on their behalf.
Each of these documents serves a unique purpose in the broader context of healthcare management, patient rights, and information privacy. Whether you're a patient, a healthcare provider, or a legal representative, understanding how these forms work together can help navigate the complex landscape of healthcare information management. The Memorial Hermann Release form is just one piece of this intricate puzzle, facilitating the lawful and consented release of health records for specified purposes.
Similar forms
A HIPAA Authorization Form is closely related to the Memorial Hermann Release form in terms of its function and goals. The HIPAA Authorization Form is used to give consent for the release of an individual's health information to specified parties for specified reasons, very much like the Memorial Hermann form which explicitly authorizes the health system to disclose health records to mentioned entities for particular purposes, such as medical care or legal needs. Both documents ensure that the release of health information complies with privacy laws while being directed by the patient's or their representative's authorization.
A Medical Consent Form bears similarity with the Memorial Hermann Release form by empowering another party to access or make decisions regarding an individual's health information or treatment. While the Memorial Hermann form specifically addresses the disclosure of health records, a Medical Consent Form might be broader, authorizing medical treatments or procedures in addition to record disclosure. Nonetheless, both forms require explicit consent from the patient or their legal representative, emphasizing the patient's control over their health information and treatments.
The Information Release Form in educational institutions also mirrors the Memorial Hermann Release form in structure and purpose. They are used to authorize the release of a student's records, like academic or health information, to specified third parties. Although one pertains to educational records and the other to health records, both require clear identification of the information to be released, the purpose of the disclosure, and to whom the information is being disclosed, safeguarding the individual's privacy rights.
Lastly, Legal Information Release Forms used by law firms or legal service providers have significant similarities with the Memorial Hermann Release form. These legal documents authorize the release and sharing of confidential information pertinent to legal matters, much like the healthcare form permits the disclosure of health records for legal purposes among others. They both necessitate detailed specifications regarding the scope and purpose of the information release, ensuring that the disclosure is directly aligned with the consent provided by the client or patient.
Dos and Don'ts
Filling out the Memorial Hermann Release form is a crucial step in managing your healthcare information. It's important to approach this process with attention to detail to ensure your medical records are handled correctly and efficiently. Here are several do's and don'ts to keep in mind:
- Do verify the mailing address for Memorial Hermann Release of Information to confirm it matches the information on the form: 7737 SWF C94 Houston, TX 77074.
- Do specify the purpose of the disclosure by checking the appropriate box such as Medical Care, Legal, Insurance, or Other, and provide a detailed explanation if you select "Other".
- Do complete the section that asks for the DATES OF SERVICE clearly and accurately. This information is crucial to ensure the correct records are released.
- Do choose the format in which you prefer to receive your medical records, whether as PAPER or via Electronic Disclosure, such as a CD.
- Do sign and date the form to give your authorization. Without your signature, the release of your medical records cannot proceed.
- Don't leave the "Specify dates" line blank. Providing specific dates ensures that only the relevant records are released, protecting your privacy.
- Don't check facilities on the form that did not provide you with services. Only authorize the release of records from facilities that you were actually treated at.
- Don't ignore the exclusions. If you wish certain information to be withheld, such as HIV Testing Only, make sure to check the appropriate box.
- Don't forget to indicate your relationship to the patient if you are not the patient yourself but are authorized to request medical records on their behalf.
Correctly filling out the Memorial Hermann Release form is a vital step in ensuring that your medical records are shared appropriately for your continued care or other necessary purposes. Attention to detail and following these guidelines can aid in avoiding delays or potential issues with the release of your Protected Health Information.
Misconceptions
When navigating the process of obtaining medical records, it's crucial to have accurate information, especially regarding specific forms like the Memorial Hermann Release form. However, several misconceptions about this form can lead to confusion. Here are five common misunderstandings clarified to assist in better grasping its use and requirements:
- Misconception 1: One form fits all locations. Despite the single mailing address listed for Memorial Hermann Release of Information, it's not a one-size-fits-all approach. The form allows for the selection of specific Memorial Hermann facilities from which to request records, indicating a tailored approach to information release based on patient needs and treatment locations.
- Misconception 2: The form is valid indefinitely. The authorization provided by signing the form is not unlimited in time. It specifies that the authorization is valid until the 180th day after signing, not to exceed 24 months, unless otherwise stated or revoked by the patient. This timeframe is crucial for ensuring the timely and relevant use of released information.
- Misconception 3: Any information can be shared without patient consent. The form explicitly requires patient or authorized representative consent for the release of records, ensuring that patient privacy is respected. The form also provides options regarding which parts of the medical record can be disclosed, showing a commitment to patient-directed information sharing.
- Misconception 4: The form automatically grants access to all medical records. Patients have the option to specifically designate the type of information to be released, including the option to exclude certain elements or to request only pertinent abstracts, specific reports, or the entire record, with special provisions for sensitive information such as HIV testing. This means that not all records are automatically accessible upon a general request; the scope must be clearly defined by the patient.
- Misconception 5: There is no cost involved in obtaining records. The form indicates that fees and charges for the release of medical records will comply with all laws and regulations, implying that costs may be incurred. Records will be released after full payment is received, highlighting the potential for financial obligations as part of the record request process.
Understanding these facets of the Memorial Hermann Release form can help in navigating the process of medical records requests more effectively, ensuring patients and their representatives manage their health information accurately and in compliance with their wishes.
Key takeaways
When completing the Memorial Hermann Release Form, it's important to understand the process and requirements to ensure accurate and timely access to medical records. Here are some key takeaways:
- Unified Mailing Address: Regardless of which facility your records are located in, there is one mailing address for all Memorial Hermann facilities that handle the release of information. This simplifies where the release form should be sent.
- Specific Authorization: The form requires that you specify the facilities you're authorizing to release your records. Only check the boxes next to the facilities where you received treatment to avoid any unnecessary release of information.
- Purpose and Format of Release: Clearly stating the purpose of the request and the preferred format of the records (paper or electronic) helps ensure that your needs are met efficiently. Whether for medical care, legal, insurance purposes, or others, specifying the reason helps the processing of your request.
- Right to Revoke: It’s crucial to know that you have the right to revoke this authorization at any time, provided you do so in writing. However, this does not affect any actions already taken based on the authorization. This ensures your control over your personal health information.
Remember to complete every required section of the form, including your name, address, date of birth, and specific dates of service you're requesting records for. Missteps in filling out the form can delay the process. Ensure you sign and date the form to validate your authorization for the release of your medical records.
Popular PDF Forms
How Do You Pay Back Unemployment - Businesses must submit this form if there have been changes in contact information, legal name, or business structure.
Secondary Leaving Certificate - Acts as a credible endorsement of Jackson Henry Agarwal's educational attainment and character for all stakeholders.
Medicaid Card Online - Free legal assistance is available for applicants needing guidance or help with the application process, ensuring access to support services.