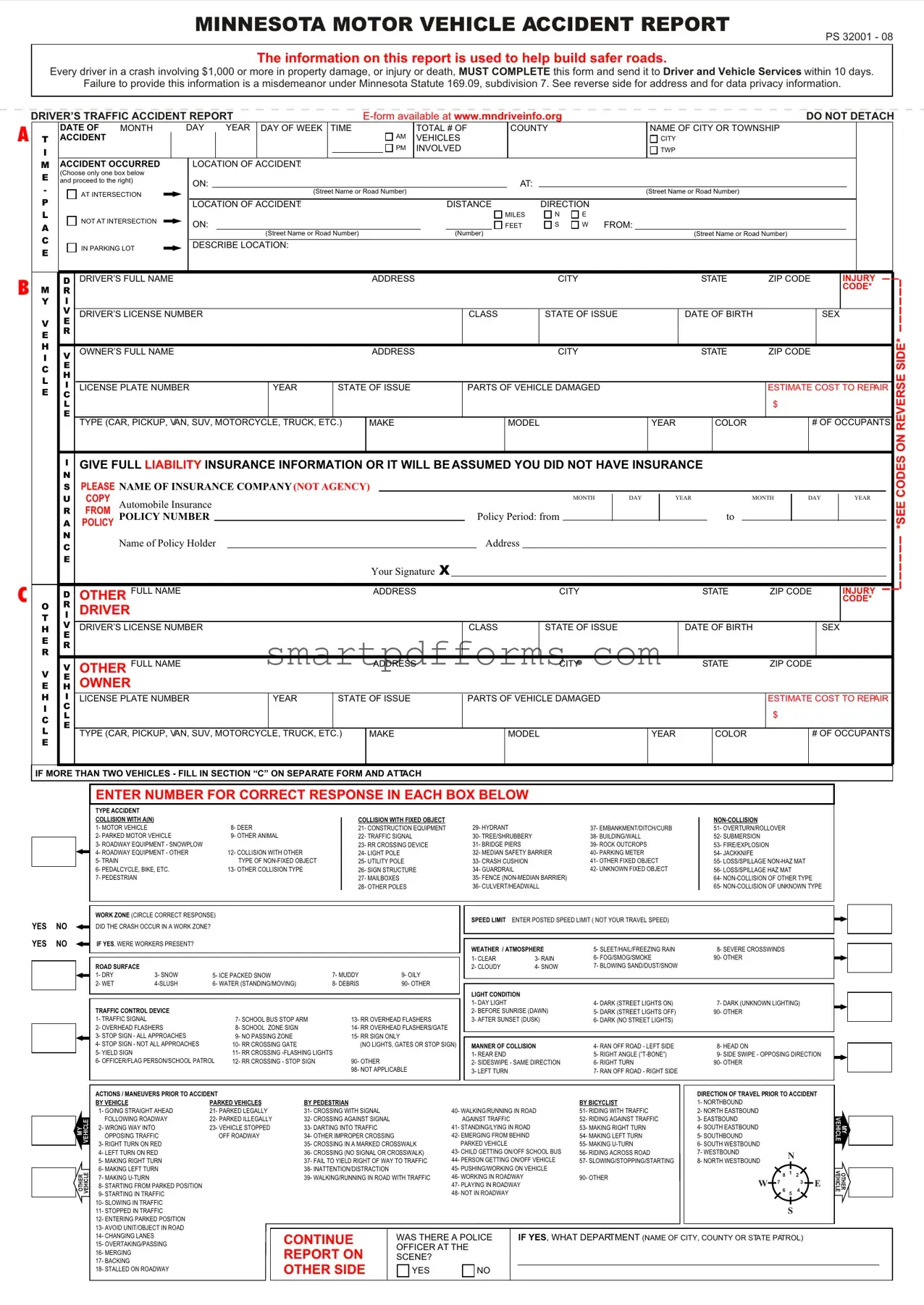
Blank Minnesota Accident Report PDF Template
In the state of Minnesota, drivers find themselves governed by a responsibility to report motor vehicle accidents promptly and accurately through the Minnesota Motor Vehicle Accident Report (PS 32001 - 08). This crucial document plays a significant role in enhancing road safety by providing essential data utilized in shaping safer roadways. The mandate stipulates that any driver involved in a crash resulting in either $1,000 or more in property damage, or any injury or death, must complete and submit this form to the Driver and Vehicle Services (DVS) no later than ten days following the incident. Neglecting this responsibility is not taken lightly, as failure to comply can lead to misdemeanor charges under Minnesota Statute 169.09, subdivision 7. The form itself is meticulously designed to gather comprehensive details about the accident, encompassing the date, location, participating vehicles, drivers’ personal information, insurance details, and a descriptive account of the event. Moreover, the form includes specific sections for detailing the accident's circumstances, such as the weather conditions, road surface, light condition, and traffic control devices present. This stringent reporting protocol underscores Minnesota’s commitment to understanding and addressing the factors contributing to road accidents, thereby fostering safer driving environments for all.
Preview - Minnesota Accident Report Form
MINNESOTA MOTOR VEHICLE ACCIDENT REPORT
PS 32001 - 08
The information on this report is used to help build safer roads.
Every driver in a crash involving $1,000 or more in property damage, or injury or death, MUST COMPLETE this form and send it to Driver and Vehicle Services within 10 days.
Failure to provide this information is a misdemeanor under Minnesota Statute 169.09, subdivision 7. See reverse side for address and for data privacy information.
A
B
C
DRIVER’S TRAFFIC ACCIDENT REPORT |
|
|
|
DO NOT DETACH |
|||||||||||||||||||||||||
|
|
DATE OF |
MONTH |
DAY |
YEAR |
DAY OF WEEK |
TIME |
|
|
TOTAL # OF |
|
COUNTY |
|
|
NAME OF CITY OR TOWNSHIP |
|
|
|
|
||||||||||
T |
|
ACCIDENT |
|
|
|
|
|
|
|
|
|
|
AM |
VEHICLES |
|
|
|
|
|
CITY |
|
|
|
|
|
||||
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
INVOLVED |
|
|
|
|
|
TWP |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
M |
|
ACCIDENT OCCURRED |
LOCATION OF ACCIDENT: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
E |
|
(Choose only one box below |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
and proceed to the right) |
ON: |
|
|
|
|
|
|
|
|
|
|
|
|
|
AT: |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
AT INTERSECTION |
|
|
|
|
(Street Name or Road Number) |
|
|
|
|
|
|
|
|
(Street Name or Road Number) |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
P |
|
|
|
|
|
LOCATION OF ACCIDENT: |
|
|
|
|
DISTANCE |
|
|
DIRECTION |
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MILES |
N |
E |
|
|
|
|
|
|
|
|
A |
|
|
NOT AT INTERSECTION |
ON: |
|
|
|
|
|
|
|
|
|
|
FEET |
S |
W FROM: |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
C |
|
|
|
|
|
|
|
|
|
(Street Name or Road Number) |
|
|
|
|
(Number) |
|
|
|
|
|
(Street Name or Road Number) |
|
|
|
|
||||
|
|
IN PARKING LOT |
DESCRIBE LOCATION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
D DRIVER’S FULL NAME |
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
|
INJURY |
||||||
M |
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CODE* |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Y |
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
V |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER’S LICENSE NUMBER |
|
|
|
|
|
|
|
|
CLASS |
|
|
STATE OF ISSUE |
|
DATE OF BIRTH |
|
SEX |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
VE
E R
H |
V |
|
OWNER’S FULL NAME |
|
|
ADDRESS |
|
CITY |
|
STATE |
ZIP CODE |
||
I |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
E |
|
|
|
|
|
|
|
|
|
|
|
|
H |
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LICENSE PLATE NUMBER |
YEAR |
STATE OF ISSUE |
PARTS OF VEHICLE DAMAGED |
|
|
|
ESTIMATE COST TO REPAIR |
||||
E |
C |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
$ |
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE (CAR, PICKUP, VAN, SUV, MOTORCYCLE, TRUCK, ETC.) |
MAKE |
|
MODEL |
YEAR |
|
COLOR |
|
# OF OCCUPANTS |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IGIVE FULL LIABILITY INSURANCE INFORMATION OR IT WILL BE ASSUMED YOU DID NOT HAVE INSURANCE
N
SPLEASE NAME OF INSURANCE COMPANY (NOT AGENCY)
|
|
U |
COPY |
Automobile Insurance |
|
|
|
|
|
|
|
|
|
|
|
|
MONTH |
|
DAY |
|
YEAR |
|
|
|
MONTH |
|
DAY |
|
YEAR |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
R |
FROM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
POLICY NUMBER |
|
|
|
|
|
|
|
|
Policy Period: from |
|
|
|
|
|
|
|
|
to |
|
|
|
|
|
|
|
|
|||||||
|
|
A |
POLICY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
Name of Policy Holder |
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Your Signature X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
D |
OTHER |
FULL NAME |
|
|
|
ADDRESS |
|
|
|
|
|
CITY |
|
|
|
|
STATE |
ZIP CODE |
|
INJURY |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CODE* |
||||
O |
|
R |
DRIVER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
T |
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
V |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H |
|
DRIVER’S LICENSE NUMBER |
|
|
|
|
|
|
CLASS |
|
STATE OF ISSUE |
|
|
|
DATE OF BIRTH |
|
|
|
|
SEX |
|||||||||||||||
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
V |
|
V |
OTHER FULL NAME |
|
|
|
ADDRESS |
|
|
|
|
|
CITY |
|
|
|
|
STATE |
ZIP CODE |
|
|
|
|||||||||||||
|
HE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
OWNER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
H |
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
LICENSE PLATE NUMBER |
|
YEAR |
STATE OF ISSUE |
|
PARTS OF VEHICLE DAMAGED |
|
|
|
|
|
|
|
|
ESTIMATE COST TO REPAIR |
||||||||||||||||||||
I |
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
C |
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE (CAR, PICKUP, VAN, SUV, MOTORCYCLE, TRUCK, ETC.) |
MAKE |
|
|
MODEL |
|
|
|
|
YEAR |
|
|
COLOR |
|
|
# OF OCCUPANTS |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
IF MORE THAN TWO VEHICLES - FILL IN SECTION “C” ON SEPARATE FORM AND ATTACH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*SEE CODES ON REVERSE SIDE*
ENTER NUMBER FOR CORRECT RESPONSE IN EACH BOX BELOW
|
|
|
|
TYPE ACCIDENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COLLISION WITH A(N) |
|
|
|
|
COLLISION WITH FIXED OBJECT |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
1- MOTOR VEHICLE |
|
|
8- DEER |
|
21- CONSTRUCTION EQUIPMENT |
29- HYDRANT |
|
37- EMBANKMENT/DITCH/CURB |
51- OVERTURN/ROLLOVER |
|
|
|
|
|
2- PARKED MOTOR VEHICLE |
|
9- OTHER ANIMAL |
|
22- TRAFFIC SIGNAL |
30- TREE/SHRUBBERY |
|
38- BUILDING/WALL |
52- SUBMERSION |
||
|
|
|
|
3- ROADWAY EQUIPMENT - SNOWPLOW |
|
|
|
23- RR CROSSING DEVICE |
31- BRIDGE PIERS |
|
39- ROCK OUTCROPS |
53- FIRE/EXPLOSION |
||
|
|
|
|
4- ROADWAY EQUIPMENT - OTHER |
|
12- COLLISION WITH OTHER |
|
24- LIGHT POLE |
|
32- MEDIAN SAFETY BARRIER |
40- PARKING METER |
54- JACKKNIFE |
||
|
|
|
|
5- TRAIN |
|
|
TYPE OF |
|
25- UTILITY POLE |
33- CRASH CUSHION |
|
41- OTHER FIXED OBJECT |
55- LOSS/SPILLAGE |
|
|
|
|
|
6- PEDALCYCLE, BIKE, ETC. |
|
13- OTHER COLLISION TYPE |
|
26- SIGN STRUCTURE |
34- GUARDRAIL |
|
42- UNKNOWN FIXED OBJECT |
56- LOSS/SPILLAGE HAZ MAT |
||
|
|
|
|
7- PEDESTRIAN |
|
|
|
|
27- MAILBOXES |
|
35- FENCE |
|
64- |
|
|
|
|
|
|
|
|
|
|
28- OTHER POLES |
36- CULVERT/HEADWALL |
|
65- |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
WORK ZONE (CIRCLE CORRECT RESPONSE) |
|
|
|
|
SPEED LIMIT ENTER POSTED SPEED LIMIT ( NOT YOUR TRAVEL SPEED) |
|
||||
YES |
NO |
|
|
|
|
|
|
|
|
|||||
DID THE CRASH OCCUR IN A WORK ZONE? |
|
|
|
|
|
|
|
|
|
|||||
YES |
NO |
IF YES, WERE WORKERS PRESENT? |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
WEATHER / ATMOSPHERE |
5- SLEET/HAIL/FREEZING RAIN |
8- SEVERE CROSSWINDS |
|||||||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
1- CLEAR |
3- RAIN |
6- FOG/SMOG/SMOKE |
90- OTHER |
|
|
|
|
ROAD SURFACE |
|
|
|
|
|
|
2- CLOUDY |
4- SNOW |
7- BLOWING SAND/DUST/SNOW |
|
|
|
|
|
1- DRY |
3- SNOW |
5- ICE PACKED SNOW |
7- MUDDY |
9- OILY |
|
|
|
|
||
|
|
|
|
2- WET |
6- WATER (STANDING/MOVING) |
8- DEBRIS |
90- OTHER |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
LIGHT CONDITION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1- DAY LIGHT |
|
4- DARK (STREET LIGHTS ON) |
7- DARK (UNKNOWN LIGHTING) |
|
|
|
|
TRAFFIC CONTROL DEVICE |
|
|
|
|
|
2- BEFORE SUNRISE (DAWN) |
5- DARK (STREET LIGHTS OFF) |
90- OTHER |
||
|
|
|
|
1- TRAFFIC SIGNAL |
|
|
7- SCHOOL BUS STOP ARM |
|
13- RR OVERHEAD FLASHERS |
3- AFTER SUNSET (DUSK) |
6- DARK (NO STREET LIGHTS) |
|
||
|
|
|
|
2- OVERHEAD FLASHERS |
|
8- SCHOOL ZONE SIGN |
|
14- RR OVERHEAD FLASHERS/GATE |
|
|
|
|
||
|
|
|
|
3- STOP SIGN - ALL APPROACHES |
|
9- NO PASSING ZONE |
|
15- RR SIGN ONLY |
|
|
|
|
|
|
|
|
|
|
4- STOP SIGN - NOT ALL APPROACHES |
|
10- RR CROSSING GATE |
|
(NO LIGHTS, GATES OR STOP SIGN) |
MANNER OF COLLISION |
4- RAN OFF ROAD - LEFT SIDE |
8- HEAD ON |
|||
|
|
|
|
5- YIELD SIGN |
|
|
11- RR CROSSING |
|
1- REAR END |
|
5- RIGHT ANGLE |
9- SIDE SWIPE - OPPOSING DIRECTION |
||
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
6- OFFICER/FLAG PERSON/SCHOOL PATROL |
12- RR CROSSING - STOP SIGN |
|
90- OTHER |
|
2- SIDESWIPE - SAME DIRECTION |
6- RIGHT TURN |
90- OTHER |
|||
|
|
|
|
|
|
|
|
|
98- NOT APPLICABLE |
3- LEFT TURN |
|
7- RAN OFF ROAD - RIGHT SIDE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MY |
VEHICLE |
OTHER |
VEHICLE |
ACTIONS / MANEUVERS PRIOR TO ACCIDENT
BY VEHICLE |
PARKED VEHICLES |
1- GOING STRAIGHT AHEAD |
21- PARKED LEGALLY |
FOLLOWING ROADWAY |
22- PARKED ILLEGALLY |
2- WRONG WAY INTO |
23- VEHICLE STOPPED |
OPPOSING TRAFFIC |
OFF ROADWAY |
3- RIGHT TURN ON RED |
|
4- LEFT TURN ON RED |
|
5- MAKING RIGHT TURN |
|
6- MAKING LEFT TURN |
|
7- MAKING |
|
8- STARTING FROM PARKED POSITION |
|
9- STARTING IN TRAFFIC |
|
10- SLOWING IN TRAFFIC |
|
11- STOPPED IN TRAFFIC |
|
12- ENTERING PARKED POSITION |
|
13- AVOID UNIT/OBJECT IN ROAD |
|
14- CHANGING LANES |
|
15- OVERTAKING/PASSING |
|
16- MERGING |
|
17- BACKING |
|
18- STALLED ON ROADWAY |
|
|
|
|
|
|
|
|
|
|
DIRECTION OF TRAVEL PRIOR TO ACCIDENT |
|||||||
BY PEDESTRIAN |
|
|
|
|
BY BICYCLIST |
1- NORTHBOUND |
|
|
|
|
|
|
|
|
31- CROSSING WITH SIGNAL |
|
40- WALKING/RUNNING IN ROAD |
51- RIDING WITH TRAFFIC |
2- NORTH EASTBOUND |
|
|
|
|
|
|
|
|||
32- CROSSING AGAINST SIGNAL |
|
AGAINST TRAFFIC |
|
52- RIDING AGAINST TRAFFIC |
3- EASTBOUND |
|
|
|
|
|
|
|
||
33- DARTING INTO TRAFFIC |
|
41- STANDING/LYING IN ROAD |
53- MAKING RIGHT TURN |
4- SOUTH EASTBOUND |
|
|
|
|
|
|
|
|||
34- OTHER IMPROPER CROSSING |
|
42- EMERGING FROM BEHIND |
54- MAKING LEFT TURN |
5- SOUTHBOUND |
|
|
|
|
|
|
|
|||
35- CROSSING IN A MARKED CROSSWALK |
PARKED VEHICLE |
|
55- MAKING |
6- SOUTH WESTBOUND |
|
|
|
|
|
|
|
|||
36- CROSSING (NO SIGNAL OR CROSSWALK) |
43- CHILD GETTING ON/OFF SCHOOL BUS |
56- RIDING ACROSS ROAD |
7- WESTBOUND |
|
|
N |
|
|
|
|||||
37- FAIL TO YIELD RIGHT OF WAY TO TRAFFIC |
44- PERSON GETTING ON/OFF VEHICLE |
57- SLOWING/STOPPING/STARTING |
8- NORTH WESTBOUND |
|
|
|
|
|
||||||
38- INATTENTION/DISTRACTION |
|
45- PUSHING/WORKING ON VEHICLE |
|
|
|
|
|
|
|
|
|
|||
|
|
|
8 |
1 |
2 |
|
|
|||||||
39- WALKING/RUNNING IN ROAD WITH TRAFFIC |
46- WORKING IN ROADWAY |
90- OTHER |
|
|
|
|||||||||
|
|
|
|
|
||||||||||
W |
|
7 |
|
|
3 |
|
E |
|||||||
|
|
|
47- PLAYING IN ROADWAY |
|
|
|
|
|
||||||
|
|
|
|
6 |
|
|
4 |
|
||||||
|
|
|
48- NOT IN ROADWAY |
|
|
|
5 |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
CONTINUE |
|
WAS THERE A POLICE |
|
IF YES, WHAT DEPARTMENT (NAME OF CITY, COUNTY OR STATE PATROL) |
|
|
||||||||
|
|
|
|
|||||||||||
|
OFFICER AT THE |
|
|
|
|
|
|
|
|
|
|
|
||
REPORT ON |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
SCENE? |
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER SIDE |
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE |
MY |
VEHICLE |
OTHER |
As required by Minnesota Data Privacy Act you are hereby informed that the information requested on this form is collected pursuant to statute to provide statistical data on traffic accidents. The time and place of the accident, names of parties involved and insurance information may be disclosed to any person involved in the accident or to others persons as specified by law. This written report cannot be used against you as evidence in any civil or criminal matter and your version of how the accident happened is confidential.
SEAT |
TYPE |
USE |
AIR BAG |
EJECT |
INJURY |
OCCUPANT SEAT POSITION CODES |
SAFETY EQUIPMENT TYPE |
RESTRAINT DEVICE USED |
SAFETY EQUIPMENT USED |
EJECTION CODES |
INJURY CODES |
|
CODES |
CODES |
CODES |
|
|
1- DRIVER |
|
|
|
1- TRAPPED, EXTRICATED |
K- KILLED |
(INCLUDE MOTORCYCLE DRIVER) |
1- NO SAFETY EQUIP IN PLACE |
1- BELTS NOT USED |
1- |
(BY MECHANICAL MEANS) |
A- INCAPACITATING INJURY |
2- FRONT CENTER |
|
2- LAP BELT ONLY USED |
2- |
2- TRAPPED, FREED BY |
B- |
3- FRONT RIGHT |
2- LAP BELT |
3- SHOULDER BELT ONLY USED |
3- |
C- POSSIBLE INJURY |
|
4- SECOND ROW SEAT LEFT |
3- SHOULDER BELT |
4- LAP AND SHOULDER BELT USED |
4- NOT |
3- PARTIALLY EJECTED |
N- NO APPARENT INJURY |
5- SECOND ROW SEAT CENTER |
4- LAP & SHOULDER BELT |
|
5- NOT |
4- EJECTED |
|
6- SECOND ROW SEAT RIGHT |
5- CHILD SAFETY SEAT |
5- CHILD SEAT NOT USED |
6- NOT DEPLOYED- UNKNOWN |
|
|
7- THIRD ROW SEAT LEFT |
6- CHILD BOOSTER SEAT |
6- CHILD SEAT USED IMPROPERLY |
IF SWITCH ON OR OFF |
5- NOT EJECTED OR TRAPPED |
|
8- THIRD ROW SEAT CENTER |
|
7- CHILD SEAT USED PROPERLY |
|
|
|
9- THIRD ROW SEAT RIGHT |
98- NOT APPLICABLE |
8- BOOSTER SEAT NOT USED |
90- OTHER DEPLOYMENTS |
|
|
10- OUTSIDE OF VEHICLE |
(MOTORCYCLE, |
9- BOOSTER SEAT USED IMPROPERLY |
98- NOT APPLICABLE |
|
|
11- TRAILING UNIT |
SNOWMOBILE, ECT.) |
10- BOOSTER SEAT USED PROPERLY |
(MOTORCYCLE, |
|
|
12- PICKUP TRUCK BED |
|
|
SNOWMOBILE, ECT.) |
|
|
13- TRUCK CAB SLEEPER SECTION |
|
11- HELMET NOT USED |
|
|
|
14- PASSENGER IN OTHER POSITION |
|
12- HELMET USED |
|
|
|
(INCLUDE MOTORCYCLE PASSENGER) |
|
|
|
|
|
15- PASSENGER IN UNKNOWN POSITION |
|
|
|
|
|
16- FRONT LEFT |
|
|
|
|
|
MY VEHICLE: DRIVER AND PASSENGERS INFORMATION: |
|
|
|
|
|
|
|
|
|
|
|
|
||
DRIVER >>>>>>>>>>>>>>>>>> |
|
DATE OF BIRTH (OR AGE) |
SEX |
SEAT |
TYPE |
USE |
AIR BAG |
EJECT |
|
|
INJURY |
|||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PASSENGER NAME |
CITY |
STATE |
|
DATE OF BIRTH (OR AGE) |
SEX |
SEAT |
TYPE |
USE |
AIR BAG |
EJECT |
|
|
INJURY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PASSENGER NAME |
CITY |
STATE |
|
DATE OF BIRTH (OR AGE) |
SEX |
SEAT |
TYPE |
USE |
AIR BAG |
EJECT |
|
|
INJURY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PASSENGER NAME |
CITY |
STATE |
|
DATE OF BIRTH (OR AGE) |
SEX |
SEAT |
TYPE |
USE |
AIR BAG |
EJECT |
|
|
INJURY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DESCRIBE ACCIDENT IN SUFFICIENT DETAIL BELOW TO DISCLOSE CAUSES. |
|
|
|
|
|
|
INDICATE |
|||||||
|
|
|
|
|
|
|
NORTH |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DESCRIBE WHAT HAPPENED: |
|
|
DIAGRAM WHAT HAPPENED: |
|
|
|
|
|
BY ARROW |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DAMAGE TO PROPERTY OTHER THAN VEHICLES: (MAILBOX, FENCE, SIGNPOST, GUARDRAIL, ETC.)
DESCRIBE |
NAME OF |
PROPERTY |
PROPERTY |
DAMAGED: |
OWNER: |
|
|
ESTIMATE COST OF REPAIR
$
SIGN HERE X
SIGNATURE OF PERSON SUBMITTING REPORT IS REQUIRED
ADDRESS |
DATE OF REPORT |
MAIL THIS REPORT TO:
DVS / ACCIDENT RECORDS
445 MINNESOTA STREET, SUITE 181
ST. PAUL, MN
Form Data
| Fact Name | Detail |
|---|---|
| Reporting Requirement | Every driver involved in a crash with $1,000 or more in property damage, or any injury or death, must complete the Minnesota Motor Vehicle Accident Report form. |
| Submission Deadline | The completed form must be sent to Driver and Vehicle Services within 10 days of the crash. |
| Legal Consequences for Non-compliance | Failure to submit this form is classified as a misdemeanor under Minnesota Statute 169.09, subdivision 7. |
| Data Privacy | Collected information is used for statistical data on traffic accidents, with certain details possibly disclosed as specified by law. The report cannot be used against the submitter in any civil or criminal case. |
Instructions on Utilizing Minnesota Accident Report
If you've been involved in a motor vehicle accident in Minnesota and the incident involved either an injury, death, or property damage of $1,000 or more, you're required to fill out the Minnesota Motor Vehicle Accident Report Form (PS 32001 - 08). It's crucial to submit this report to the Driver and Vehicle Services (DVS) within 10 days of the accident. A thorough and accurate completion of this report is not just a legal obligation, it also contributes to traffic safety analysis and the development of safer roads. Here's a step-by-step guide to help you fill out the report correctly.
- Start with your accident details. Write the date (month, day, year) and time, including AM or PM, at the top of the form. Also, note the day of the week it occurred and the total number of vehicles involved.
- Specify the county and the name of the city or township where the accident took place.
- Identify the location of the accident by choosing one of the boxes. If it was at an intersection, provide the street names or road numbers of the intersection. If not at an intersection, indicate the distance and direction from the nearest street or road number, and if in a parking lot, describe the location.
- Continue with your personal information. Enter your full name, address, city, state, and ZIP code.
- Document your driver’s license number, the state it was issued in, your date of birth, and gender.
- Fill in the vehicle owner’s details, if different from the driver, including full name, address, city, state, and ZIP code.
- Input the vehicle’s details: license plate number, year, state of issue, estimated cost to repair any damages, and type (e.g., car, SUV, motorcycle). Include the make, model, year, and color.
- Provide full liability insurance information: name of the insurance company, policy number, and the policy period dates.
- If there was another vehicle involved, repeat the above steps (5 to 8) to include the other driver’s and vehicle owner’s information, as well as their vehicle’s details and insurance information.
- For accidents involving more than two vehicles, use section “C” on a separate form and attach it.
- Select from the numbered codes to describe the accident type, including collision with another motor vehicle, collision with a fixed object, or non-collision.
- Circle the correct response regarding the work zone, and fill in the posted speed limit at the scene of the crash.
- Select the appropriate weather, road surface, and light conditions at the time of the accident.
- Mark the traffic control device present at the scene, if any.
- Choose the manner of collision from the options provided.
- Detail the actions or maneuvers prior to the accident for both your vehicle and the other vehicle involved.
- Include direction of travel prior to the accident for pedestrians or bicyclists, if applicable.
- If a police officer was at the scene, mark “Yes” and provide the department name. If not, mark “No”.
- Use the diagram area to sketch how the accident happened, using an arrow to indicate north.
- Describe the accident in detail in the space provided, clearly indicating causes and circumstances.
- List any damage to property other than vehicles, specifying the name of the property owner and an estimate of the repair cost.
- Sign and date the report at the bottom.
- Mail the completed report to the address provided on the form: DVS / Accident Records, 445 Minnesota Street, Suite 181, St. Paul, MN 55101-5181.
Remember, your report's accuracy is essential not just for legal compliance but for contributing valuable data towards efforts to improve road safety. Make sure to provide as much detail as possible and review your report before submission to ensure clarity and completeness.
Obtain Answers on Minnesota Accident Report
Who needs to complete the Minnesota Motor Vehicle Accident Report?
Where can I find the Minnesota Motor Vehicle Accident Report form?
What is the deadline for submitting the Minnesota Motor Vehicle Accident Report?
What happens if I don’t submit the accident report?
What should I include in the accident report?
Can the information I provide in the report be used against me?
Who can access the information in my accident report?
How should I describe the accident on the report?
What if there were more than two vehicles involved?
Where do I send the completed Minnesota Motor Vehicle Accident Report?
Any driver involved in a crash resulting in either $1,000 or more in property damage, personal injury, or death must complete the Minnesota Motor Vehicle Accident Report form.
The form is accessible online at www.mndriveinfo.org. You can download the E-form from this website.
You must send the completed form to Driver and Vehicle Services within 10 days following the accident.
Failure to submit the report when required is a misdemeanor under Minnesota Statute 169.09, subdivision 7. This legal responsibility underscores the importance of timely submission to avoid potential legal consequences.
You'll need to include detailed information about the accident, including the date, time, location, driver and vehicle details, a description of what happened, and any property damage or injuries. Additionally, it's crucial to provide full liability insurance information.
No, the information you submit in this report, specifically your version of how the accident occurred, is confidential and cannot be used against you in any civil or criminal matter according to the Minnesota Data Privacy Act.
While your narrative of the accident is protected, other details like the time and place of the accident, names of parties involved, and insurance information may be disclosed to those involved in the accident or other specified persons by law.
Provide a clear and detailed description of the accident, including how it happened, the direction and speed of the vehicles, actions taken by the drivers before the accident, weather conditions, and any other relevant information. Use the diagram section to visually explain the accident layout.
If the crash involved more than two vehicles, fill out section “C” on additional forms and attach them to your report to provide comprehensive details about all vehicles and drivers involved.
Mail your completed report to: DVS / Accident Records, 445 Minnesota Street, Suite 181, St. Paul, MN 55101-5181.
Common mistakes
When filling out the Minnesota Accident Report form, certain common mistakes can lead to delays or inaccuracies in processing. Here is an overview of some of these errors:
- Not reporting within the 10-day window: All drivers involved in a crash with $1,000 or more in property damage, or any injury or death, must submit the form to Driver and Vehicle Services within 10 days. Failing to do this can result in a misdemeanor charge.
- Incomplete insurer information: It's crucial to provide full liability insurance information. If this section is incomplete, it may be assumed that the driver did not have insurance coverage at the time of the accident.
- Omitting accident location details: The form requires specific information regarding where the accident occurred, including whether it was at an intersection and the direction from a landmark. Leaving these details vague can impede investigations.
- Unclear accident description: A clear and thorough description of the accident helps in understanding the circumstances. Descriptions lacking sufficient detail fail to provide a complete picture of the incident.
- Incorrect or missing vehicle information: Including the make, model, year, and color of the vehicle, as well as the license plate number and state of issue, is mandatory. Incorrect or missing data can complicate record-keeping and follow-ups.
- Not detailing damage to vehicles: It's important to list the parts of the vehicle that were damaged and provide an estimate of the repair costs. Failure to do so can complicate insurance claims.
- Leaving injury codes blank: If injuries occurred, the proper injury codes must be used to describe their severity. Not using these codes, or using them incorrectly, may impact insurance or legal outcomes.
- Forgetting to list passengers: All passengers, along with their seat positions and any injuries sustained, need to be accounted for in the report. This information is crucial for insurance and legal purposes.
- Failing to sign the report: The report requires the signature of the person submitting it. An unsigned report is considered incomplete and cannot be processed.
Accuracy and completeness when filling out this form are vital for ensuring a smooth process with insurance claims and legal proceedings, and for contributing to safer roadways by providing accurate data for statistical analysis.
Documents used along the form
When involved in a motor vehicle accident in Minnesota, individuals may need to complete and provide additional forms and documents along with the Minnesota Accident Report form. These supplementary documents play a crucial role in ensuring a comprehensive account of the incident is recorded, facilitating insurance claims, and promoting road safety. Understanding these documents can greatly assist in navigating the aftermath of an accident.
- Insurance Policy Document: This document verifies the insurance coverage of the vehicle(s) involved in the accident. It typically includes the insurance company's name, the policy number, and the coverage period, which are essential for filing insurance claims.
- Medical Records: In cases where injuries have occurred due to the accident, medical records are critical. They provide a detailed account of the injuries sustained, treatments received, and the prognosis, which is vital for insurance claims and legal proceedings.
- Vehicular Repair Estimates: After an accident, repair estimates from certified mechanics or auto repair shops document the extent of the damage and the expected costs to restore the vehicle. These estimates are crucial for insurance claim processes.
- Witness Statements: Statements from individuals who witnessed the accident can be pivotal in establishing the events leading up to, during, and following the collision. These are often used to corroborate the accounts provided by the drivers involved.
- Photographic Evidence: Photos taken at the accident scene, including those of the vehicles, location, and any relevant road signs or conditions, provide visual documentation that can support claims and reports.
- Police Report: If law enforcement attended the scene of the accident, a police report might be generated. This report offers an authoritative third-party perspective on the accident, including observations on fault, violations, and other critical details.
Together, these documents complement the Minnesota Accident Report form, creating a thorough and accurate record of the accident. This comprehensive documentation is invaluable for insurance claims, legal matters, and measures aimed at preventing future accidents. Handling the aftermath of a vehicle accident can be challenging, but having the correct forms and documents organized can significantly ease the process for all parties involved.
Similar forms
Workers' Compensation Claim Form: Similar to the Minnesota Accident Report form, a Workers' Compensation Claim Form collects detailed information about an incident – including details about the individuals involved, the date, time, and location of the incident, and a description of the injury. Both forms are integral in the aftermath of an event; one addresses vehicular accidents while the other focuses on workplace injuries. Each serves as a first step in a formal process to assess and address damages or injuries sustained.
Property Damage Report Form: This document shares similarities with the Minnesota Accident Report form in that it documents specifics about incidents leading to property damage. It requires information on the location, extent of damage, parties involved, and any witness statements. Both forms are crucial for the involved parties and authorities to evaluate the circumstances and take necessary actions or provide compensation accordingly.
Police Incident Report Form: The Minnesota Accident Report form has traits in common with a Police Incident Report Form. Both collect detailed evidence about incidents – including participant information, precise locations, dates, and descriptions of the event. These documents are essential for legal and insurance purposes, helping to establish facts and allocate responsibility in a structured manner.
Insurance Claim Form: Like the Minnesota Accident Report, an Insurance Claim Form is designed to gather detailed information following an incident, which in this case is necessary for filing a claim with an insurance company. It requires specific details about the incident, including personal particulars, a narrative of what occurred, and an account of damages or injuries. Both types of forms are critical in the process of assessing claims and determining eligibility for coverage.
Vehicle Inspection Form: Though its primary purpose is different, a Vehicle Inspection Form bears similarities to the Minnesota Accident Report form in its detailed enumeration of vehicle conditions. Both require information on the make, model, and year of vehicles, alongside any damages present – be it from an accident or general wear and tear. These forms help in evaluating the state of a vehicle either post-accident or during routine checks to ensure road safety.
Dos and Don'ts
When it comes to filling out the Minnesota Accident Report form, it is crucial to provide accurate and complete information. This document is vital for insurance claims, legal reasons, and for helping to make roads safer. Here are some key dos and don'ts to keep in mind:
Do:- Report the accident promptly. Ensure you fill out and submit this form within 10 days of the accident if it involves $1,000 or more in property damage, or if there was any injury or death. This is a legal requirement.
- Provide detailed information. Use the space provided to give a thorough description of the accident. Include all relevant details such as the direction of travel, what each vehicle was doing at the time of the accident, and weather conditions. This helps in understanding the dynamics of the accident.
- Be honest and factual. Only report what actually happened, without speculation or bias. Your account should be truthful and based on facts, as this information could be used in legal proceedings or for insurance purposes.
- Review your information. Before submitting the report, double-check all the information you've entered for accuracy. This includes names, dates, insurance details, and the specifics of the accident.
- Include insurance information. Make sure to provide full liability insurance information. If this is not included, it could be assumed that you did not have insurance at the time of the accident.
- Delay submitting the form. Failing to submit the accident report within the stipulated timeframe can lead to legal consequences, such as misdemeanors under Minnesota Statute 169.09, subdivision 7.
- Leave sections blank. If a section of the form applies to your situation, ensure you fill it out completely. Incomplete information can lead to delays or issues with processing the report.
- Guess on details. If you're unsure about certain aspects of the accident, it's better to clarify or confirm the information instead of making guesses. Incorrect information could affect the outcomes of insurance claims or legal processes.
- Include unnecessary personal opinions. Stick to the facts of what happened during the accident. Personal opinions or irrelevant details may complicate the assessment of the accident.
- Forget to sign the report. Your signature is required at the bottom of the form. This certifies that the information you provided is accurate to the best of your knowledge. A missing signature can invalidate the report.
Misconceptions
There are several misconceptions about the Minnesota Motor Vehicle Accident Report Form, PS 32001 - 08, that need to be addressed for better understanding and compliance:
It's only for severe accidents: A common misconception is that the form is only necessary for severe accidents. In reality, every driver involved in a crash with $1,000 or more in property damage, or any injury or death, must complete this form.
Submission is optional: Some people believe submitting this form is optional. However, drivers must submit this form to Driver and Vehicle Services within 10 days of the accident. Failure to do so is considered a misdemeanor under Minnesota statute 169.09, subdivision 7.
Insurance information is optional: Leaving the insurance section blank because you think it's optional can lead to the assumption that you did not have valid insurance at the time of the accident, which can lead to further legal complications.
Police reports substitute the need for this form: Even if a police officer reports the crash, drivers must still complete and submit this form themselves. Police reports and this form serve different purposes and are used by different entities.
Details on the form can be used against you in court: The information provided on this form is used statistically to help build safer roads and cannot be used against you as evidence in any civil or criminal matter. Additionally, drivers' descriptions of how the accident happened are confidential.
The form is complicated and requires legal assistance: While the form is detailed, it is designed for drivers to complete without the need for legal assistance. It includes codes and instructions on the reverse side to aid in filling out the form accurately.
Only at-fault drivers must file the form: Both drivers involved in an accident with the specified damages or injuries are required to submit the form, regardless of who is at fault.
It’s not necessary to report if no injuries are visible: If there is property damage of $1,000 or more, the form must be submitted even if no injuries are apparent at the scene. Injuries can sometimes become apparent only after the accident.
You can only submit the form by mail: While the form instructions provide a mailing address, there is also an e-form available at www.mndriveinfo.org, offering an online submission option for users with internet access.
The form doesn't need to be filed if the accident occurs in a parking lot: Accidents that occur in parking lots and meet the reporting criteria (injury, death, or property damage of $1,000 or more) must also be reported using this form. Location does not exempt one from reporting.
Key takeaways
Filling out the Minnesota Accident Report form correctly is crucial for drivers in Minnesota who find themselves in a crash involving $1,000 or more in property damage, or any injury or death. This guide provides key insights to ensure that individuals complete this form accurately and comply with legal obligations.
Every driver involved in a crash that results in either $1,000 or more in property damages, any injury, or death, is mandated to fill out the Minnesota Motor Vehicle Accident Report form and submit it to Driver and Vehicle Services within 10 days. This requirement aims to gather data to enhance road safety and adherence is enforced by law under Minnesota Statute 169.09, subdivision 7.
Failure to provide the requested information on the Minnesota Accident Report form is classified as a misdemeanor. It is imperative that all sections of the form are completed fully and accurately to avoid legal repercussions and ensure a thorough documentation of the incident for statistical purposes.
The form includes sections for detailed information about the accident such as the date, time, location, type of accident, vehicles involved, and personal details of the drivers and owners of those vehicles. Accurate and comprehensive completion of these sections is essential for a meaningful evaluation of the crash data to support the development of safer roads.
Insurance information is a critical component of the report. Drivers must provide complete liability insurance details. Failure to do so will lead to an assumption of non-insurance, which could result in further legal and financial complications.
The section on the back of the form offers guidance on how to specify the type of accident, weather conditions, road surface, light conditions, and more. This information is pivotal in analyzing the contributing factors to accidents and formulating strategies to prevent similar occurrences in the future.
As stated in the Minnesota Data Privacy Act, the information collected on this form is used for statistical data on traffic accidents. The form's data concerning the time and place of the accident, involved parties' names, and insurance information may be disclosed to involved persons or others as specified by law, highlighting the importance of accuracy in filling out the form.
It is also important to note that the report’s details, including the driver's account of the accident, are treated as confidential and cannot be used as evidence in any civil or criminal matter against the person submitting the report. This provision encourages transparency and accuracy in reporting.
Popular PDF Forms
Philhealth Registration Online - Your PIN is a permanent and unique identifier within the PhilHealth system, ensuring secure and streamlined access to benefits.
Ky Purchase Exemption Certificate - A certificate required for tax-free transactions by qualified Kentucky entities.
Imm 1344 Form 2023 Pdf - The form requires sponsors to disclose any change in marital status and provide evidence if applicable.