Blank Mv 402 PDF Template
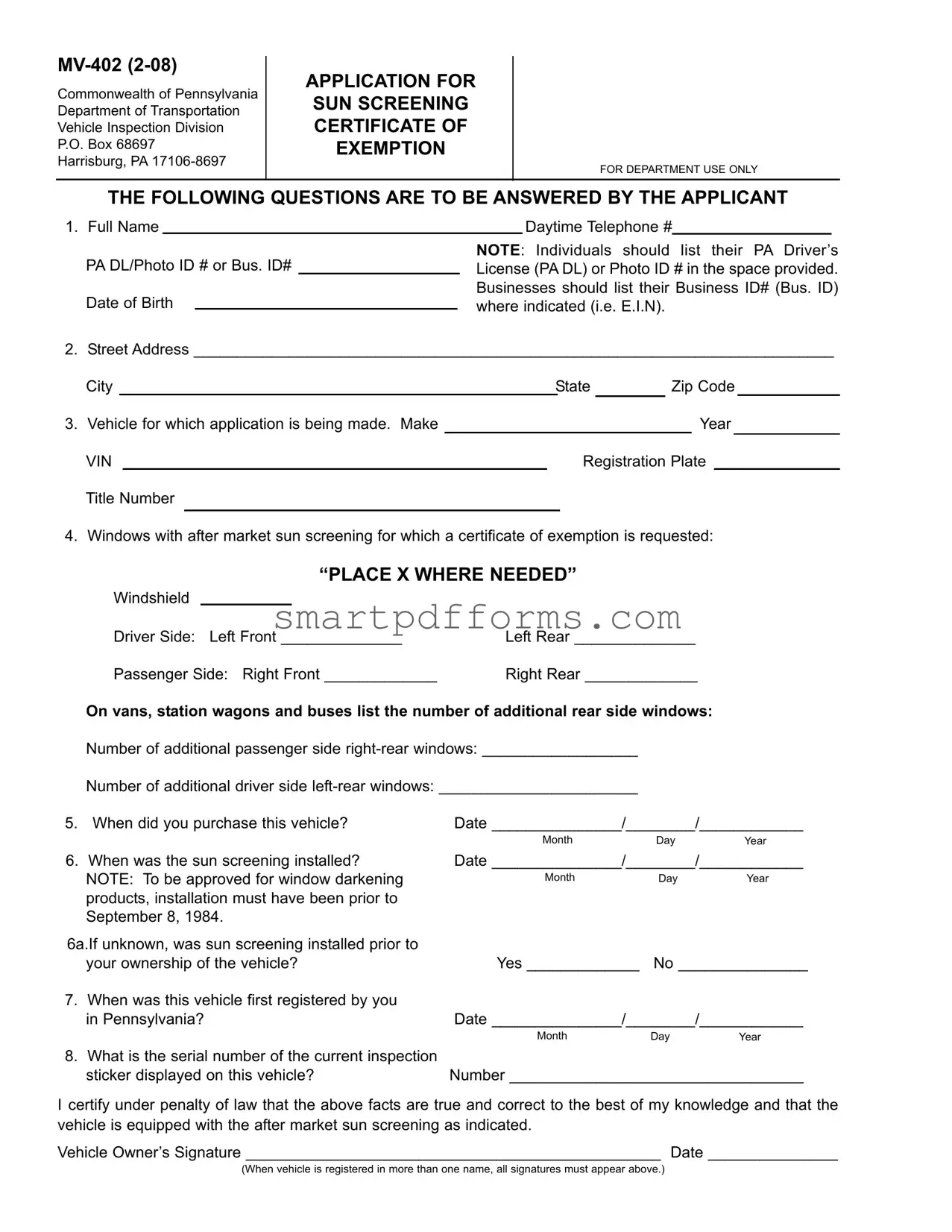
In Pennsylvania, individuals seeking to equip their vehicles with aftermarket sun screening that deviates from standard regulations must navigate the guidelines established by the Commonwealth's Department of Transportation Vehicle Inspection Division. The MV-402 form plays a crucial role in this process, serving as the "Application for Sun Screening Certificate of Exemption." This document is necessary for individuals who require darker window tints for medical reasons or other special exemptions. The form requires detailed information from the applicant, including personal identification, vehicle specifics, and the specifics of the sun screening in question. It also mandates a section to be filled out by a licensed physician or optometrist, attesting to the medical need for such an exemption. The intricacies of the MV-402 span from basic applicant identification to the technical details of the sun screening installation, including when and where the sun screening was installed, to ensure compliance with state laws that generally restrict such modifications unless a valid exemption is warranted. As such, this form is a critical step for Pennsylvania residents seeking to legally apply sun screening products that filter ultraviolet rays for health-related reasons, making it essential for vehicle owners and medical professionals to understand its requirements and implications thoroughly.
Preview - Mv 402 Form
Commonwealth of Pennsylvania
Department of Transportation
Vehicle Inspection Division
P.O. Box 68697
Harrisburg, PA
APPLICATION FOR SUN SCREENING CERTIFICATE OF EXEMPTION
FOR DEPARTMENT USE ONLY
THE FOLLOWING QUESTIONS ARE TO BE ANSWERED BY THE APPLICANT
1. Full Name
PA DL/Photo ID # or Bus. ID#
Date of Birth
Daytime Telephone #
NOTE: Individuals should list their PA Driver’s License (PA DL) or Photo ID # in the space provided. Businesses should list their Business ID# (Bus. ID) where indicated (i.e. E.I.N).
2. |
Street Address __________________________________________________________________________ |
||||||||||||
|
City |
|
|
State |
|
Zip Code |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
Vehicle for which application is being made. Make |
|
|
|
|
|
|
Year |
|||||
|
VIN |
|
|
|
|
Registration Plate |
|
|
|||||
|
Title Number |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. Windows with after market sun screening for which a certificate of exemption is requested:
“PLACE X WHERE NEEDED”
Windshield |
|
|
|
Driver Side: Left Front ______________ |
Left Rear ______________ |
||
Passenger Side: Right Front _____________ |
Right Rear _____________ |
||
On vans, station wagons and buses list the number of additional rear side windows:
|
Number of additional passenger side |
|
|
|
|
Number of additional driver side |
|
|
|
5. |
When did you purchase this vehicle? |
Date _______________/________/____________ |
||
|
|
Month |
Day |
Year |
6. |
When was the sun screening installed? |
Date _______________/________/____________ |
||
|
NOTE: To be approved for window darkening |
Month |
Day |
Year |
|
products, installation must have been prior to |
|
|
|
|
September 8, 1984. |
|
|
|
6a.If unknown, was sun screening installed prior to |
|
|
|
|
|
your ownership of the vehicle? |
Yes _____________ |
No _______________ |
|
7. When was this vehicle first registered by you |
|
|
|
|
|
in Pennsylvania? |
Date _______________/________/____________ |
||
|
|
Month |
Day |
Year |
8. What is the serial number of the current inspection |
|
|
|
|
|
sticker displayed on this vehicle? |
Number __________________________________ |
||
I certify under penalty of law that the above facts are true and correct to the best of my knowledge and that the vehicle is equipped with the after market sun screening as indicated.
Vehicle Owner’s Signature ________________________________________________ Date _______________
(When vehicle is registered in more than one name, all signatures must appear above.)
REQUEST FOR MEDICAL EXEMPTION
This portion must be completed by a licensed physician or optometrist when a certificate of exemption is requested due to a physical condition. NOTE: The exemption is valid only for colorless sun screening products that filter ultraviolet rays.
(Please type or print)
PATIENT INFORMATION
Patient Name ___________________________________________ Daytime Telephone # _________________
Street Address _____________________________________________________________________________
City ___________________________________________________ State __________ Zip Code ___________
Brief Description of patients condition: ___________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
Suggested Treatment(s): _____________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
PHYSICIAN/OPTOMETRIST INFORMATION
Physician/Optometrist Name ___________________________________________________
Business Affiliation (if any) _____________________________________________________
Business Address ____________________________________________________________
City ___________________________________________ State _____ Zip Code _________
Physician Telephone Number __________________________________________________
I certify under penalty of law that the above facts are true and correct to the best of my knowledge:
Signature _______________________________________ Date _____________________
THE REVERSE SIDE MUST BE COMPLETED BY THE VEHICLE OWNER
Form Data
| Fact Name | Description |
|---|---|
| Form Title | Application for Sun Screening Certificate of Exemption |
| Issuing Body | Commonwealth of Pennsylvania Department of Transportation Vehicle Inspection Division |
| Form Number and Revision Date | MV-402 (2-08) |
| Submission Address | P.O. Box 68697, Harrisburg, PA 17106-8697 |
| Eligibility for Application | Individuals must use their PA Driver's License (PA DL) or Photo ID number, Businesses must use their Business ID Number (Bus. ID). |
| Sun Screening Installation Date Requirement | To be approved, sun screening products must have been installed prior to September 8, 1984. |
| Medical Exemption Requirement | A licensed physician or optometrist must complete the request for medical exemption due to a physical condition. |
| Governing Law | Pennsylvania vehicle inspection regulations |
| Serial Number Requirement | The serial number of the current inspection sticker displayed on the vehicle must be provided. |
Instructions on Utilizing Mv 402
Applying for a sun screening certificate of exemption requires attention to detail, as this process involves providing accurate vehicle and personal information, alongside medical documentation if necessary. The MV-402 form is integral for those seeking permission to use darker tint levels due to medical conditions. Completing this form involves a series of straightforward steps. Below, you'll find a guide designed to assist in filling out the form accurately, ensuring all necessary details are provided and compliance with the Department of Transportation's requirements.
- Begin with your personal details. Enter your Full Name and either your PA Driver’s License (PA DL)/Photo ID number in the space provided or, if a business entity, enter the Business ID# (E.I.N).
- Provide your Street Address, including city, state, and zip code.
- Fill in the details of the vehicle for which the application is being made. This includes the make, year, VIN, registration plate, and title number.
- Identify which windows have aftermarket sun screening installed. Place an “X” in the appropriate boxes to denote the windshield, driver side, and passenger side windows, including any additional rear side windows for vans, station wagons, and buses.
- Indicate the date of purchase of the vehicle, ensuring to fill out the month, day, and year.
- Specify the date the sun screening was installed. Remember, to qualify for a certificate, the installation must have occurred prior to September 8, 1984. If unknown, indicate whether the screening was installed before you took ownership of the vehicle.
- Provide the date the vehicle was first registered by you in Pennsylvania.
- Enter the serial number of the current inspection sticker displayed on this vehicle.
- Conclude the applicant section by signing and dating the form. If the vehicle is registered in more than one name, all owners must provide their signatures.
- If applying for a medical exemption, the REQUEST FOR MEDICAL EXEMPTION section must be completed by a licensed physician or optometrist. This includes the patient information, a brief description of the patient's condition, suggested treatments, and the physician/optometrist's information and certification.
After completing these steps, double-check your responses for accuracy and completeness. Ensuring that all sections applicable to your situation have been accurately filled out will facilitate a smoother review process. Upon submission, your application will undergo evaluation to verify its eligibility for an exemption. Proper documentation and adherence to the outlined requirements are crucial for a successful application.
Obtain Answers on Mv 402
- What is the MV-402 form and who needs to complete it?
The MV-402 form is an application for a Sun Screening Certificate of Exemption in the Commonwealth of Pennsylvania. It should be completed by individuals or businesses who wish to receive an exemption from the state's standard window tint regulations. This exemption is typically requested due to medical necessity, requiring the use of colorless sun screening products that filter ultraviolet rays. Vehicle owners who have installed aftermarket sun screening on their windows and require an exemption due to a medical condition are required to complete this form.
- What information is required when filling out the MV-402 form?
To successfully complete the MV-402 form, applicants need to provide a comprehensive set of information, including:
- The full name of the applicant, along with their PA Driver’s License (PA DL), Photo ID number, or Business ID (Bus. ID) for businesses.
- Contact information, including street address, city, state, and zip code.
- Detailed vehicle information for which the exemption is being requested, such as make, year, VIN, registration plate, and title number.
- Specific details about the aftermarket sun screening installed, including the windows that have been tinted and the date of installation.
- The date the vehicle was first registered in Pennsylvania and the current inspection sticker serial number.
This form also includes a section for a licensed physician or optometrist to fill out, confirming the medical necessity for the exemption.
- Can any tinted window be approved for exemption?
No, not all tinted windows can be approved for an exemption. To be eligible for an exemption, the sun screening installed must be colorless and capable of filtering ultraviolet rays. Furthermore, the installation of the window darkening products must have occurred prior to September 8, 1984, for the vehicle to qualify for exemption due to medical reasons. This requirement underlines the importance of providing accurate installation dates when applying for a certificate.
- What happens if I don’t know when the sun screening was installed?
If you are unsure about when the sun screening was installed on your vehicle, the form allows you to indicate this uncertainty. Specifically, question 6a asks if the sun screening was installed prior to your ownership of the vehicle. Answering 'Yes' or 'No' to this question helps the Department of Transportation understand the circumstances, although it may impact the approval for an exemption based on the age requirement for the installation of the sun screening products.
- Do both vehicle owners need to sign the MV-402 form if the vehicle is registered in multiple names?
Yes, when a vehicle is registered in more than one name, all registered owners must sign the MV-402 form. This requirement ensures that all parties are informed of and consent to the application for a sun screening certificate of exemption. Failure to obtain all necessary signatures may result in delays or the denial of the exemption request.
Common mistakes
Filling out the MV-402 form, an Application for Sun Screening Certificate of Exemption in Pennsylvania, involves providing detailed information to the Department of Transportation. Common mistakes can lead to delays or denial of the application. Knowing what errors to avoid can streamline the process and improve the chances of approval.
Incorrect Identification Numbers: Applicants often mistakenly enter invalid PA Driver’s License (PA DL), Photo ID numbers, or Business ID numbers. It is crucial to double-check these numbers for accuracy to ensure the application is processed without delay.
Omitting Required Vehicle Information: Some applicants leave sections related to the vehicle, such as make, year, VIN, registration plate, and title number blank. This information is essential for identifying the vehicle needing the sun screening exemption.
Improperly Indicating Windows for Exemption: Failing to clearly mark the windows that require sun screening exemption is a common mistake. It's important to "PLACE X WHERE NEEDED" accurately to identify the specific windows that the exemption request covers.
Inaccurate Sun Screening Installation Date: Applications must include the correct date of sun screening installation. Noting that installations must have been completed prior to September 8, 1984, for approval, providing an incorrect date can invalidate your request.
Misidentifying the Registration Date: The date when the vehicle was first registered by the applicant in Pennsylvania is often inaccurately reported or left blank. This date is pivotal for processing the application.
Failing to Include All Vehicle Owner’s Signatures: When the vehicle is registered in more than one name, all owners must sign the application. Overlooking this requirement can cause unnecessary processing delays.
Physician or Optometrist Section Incompleteness or Errors: The section of the form that must be completed by a licensed physician or optometrist is frequently filled out incorrectly or left incomplete. This section is vital for those requesting an exemption due to a physical condition, and any mistakes can lead to the rejection of the application.
By avoiding these seven mistakes, applicants can ensure their MV-402 form is accurately completed, which will facilitate a smoother review process by the Pennsylvania Department of Transportation.
Documents used along the form
When applying for a Sun Screening Certificate of Exemption in Pennsylvania, using the MV-402 form, individuals or businesses may need to accompany this application with several other forms or documents to ensure compliance with all the legal requirements set forth by the Department of Transportation. Highlighted below are six frequently required or utilized documents during this process.
- Title Certificate: This is the official document proving ownership of the vehicle. It includes important details such as the vehicle’s make, model, year, and VIN (Vehicle Identification Number), which must match the information provided on the MV-402 form.
- Proof of Insurance: Applicants must provide evidence of valid vehicle insurance. This documentation should display the name of the insurance company, the policy number, and the effective dates of coverage. Insurance ensures that the vehicle is legally covered for use on roads.
- Driver’s License: A valid Pennsylvania Driver’s License or Photo ID must be presented. This serves as proof of identity for the individual applying for the exemption and links them to the vehicle in question.
- Vehicle Registration: Current vehicle registration demonstrates that the vehicle is legally registered in Pennsylvania under the applicant's name or business name. This document contains details like the vehicle’s registration plate and title number, which should correspond to the MV-402 application.
- Physician or Optometrist Documentation: When the exemption is requested due to a physical condition, a letter or official document from a licensed physician or optometrist must accompany the MV-402. This document should describe the patient's condition and the necessity for sun screening, certifying that it's a medical requirement.
- Inspection Reports: Recent vehicle inspection documents may be required to verify that the vehicle meets Pennsylvania’s safety and emissions standards. This might be especially relevant if aftermarket sun screening could potentially affect visibility.
Together, these documents support the MV-402 application, ensuring that all requests for a Sun Screening Certificate of Exemption meet the legal prerequisites. By providing a comprehensive packet that includes these essential forms and documents, applicants can facilitate a smoother and more efficient review process.
Similar forms
The MV-402 form, as a vehicle-related legal document, shares similarities with other official forms used within various governmental and administrative contexts. These documents serve a variety of purposes, from registration and certification to applications for exemptions and permits. Here is a list of documents that bear resemblance to the MV-402 form in function and structure:
- Vehicle Registration Application: Similar to the MV-402, this form is used for registering a vehicle with a state's Department of Motor Vehicles (DMV) or similar agency. It requires personal information, vehicle details, and insurance information.
- Driver's License Application: This document is necessary for individuals seeking to obtain or renew a driver's license. It shares the need for detailed personal information and, in some cases, medical information to ensure the applicant's eligibility.
- Disability Parking Placard Application: Like the MV-402's section for a medical exemption, this form often requires a certification by a medical professional to prove the applicant's need for special parking privileges.
- Business License Application: For individuals or entities looking to start or operate a business legally within a jurisdiction. This form typically requires identification information similar to the business ID number mentioned in the MV-402.
- Title Transfer Form: Used when the ownership of a vehicle is changing hands, requiring information about the vehicle, such as make, year, and VIN, similar to the MV-402.
- Building Permit Application: Although not vehicle-related, it parallels the MV-402 in requiring specific detail submission to a government authority for review and approval before proceeding with a project or modification.
- Application for Employment: This form collects personal information, qualifications, and, occasionally, medical information to determine eligibility for a position, reflecting the personal and vehicle information blend seen in MV-402.
- Firearm Purchase Permit Application: Requires personal identification, background information, and sometimes medical information, drawing parallels with the comprehensive identification and certification process seen in the MV-402.
- Passport Application: Needs detailed personal information, proof of citizenship, and sometimes additional documentation for identity verification, similar to the personal information verification step in the MV-402 process.
- Application for Environmental Permit: Often requires detailed information about the project or operation seeking approval, including potential environmental impacts, which mirrors the detail-oriented and regulated nature of the MV-402 form for sun screening exemption.
Each of these documents, while serving distinct purposes, requires a thorough collection of personal, vehicle, business, or project information for review by respective authorities, emphasizing the structured and regulated approach to formal applications and permissions akin to the MV-402 form.
Dos and Don'ts
Filling out the MV-402 form, an Application for Sun Screening Certificate of Exemption in Pennsylvania, requires careful attention to detail. The process involves providing accurate information about the vehicle and the applicant to obtain an exemption for window tinting laws due to medical necessity. Here are important do's and don'ts to consider:
Do's:- Read the form thoroughly before starting to fill it out. This ensures understanding of all requirements and helps gather all the necessary information.
- Use black or blue ink to fill out the form to ensure clarity and longevity of the text.
- Provide accurate vehicle information, including the make, year, VIN, registration plate, and title number. This information is critical for identifying the specific vehicle that the exemption applies to.
- Clearly mark the windows that have aftermarket sun screening installed. It’s important to specify each window to avoid any confusion during the exemption process.
- Include the exact dates of vehicle purchase, sun screening installation, and first registration in Pennsylvania. Approximations can lead to delays or rejections.
- Ensure that the application is signed by all registered vehicle owners. Missing signatures can invalidate the application.
- Don't leave any fields blank. If a section does not apply, mark it with “N/A” (Not Applicable) instead of leaving it empty to indicate that the question was read and answered consciously.
- Avoid guessing details about your vehicle or sun screening. Incorrect information can lead to processing delays or denial of the application.
- Don't submit the form without the physician or optometrist’s section completed if applying for a medical exemption. This part is crucial for verifying the medical necessity of the sun screening exemption.
- Refrain from using correction fluid or tape for mistakes. If errors are made, it's better to start with a new form to maintain the document’s readability and professionalism.
- Don't forget to check the installation date of the sun screening against the required timeline. Sun screening installed after September 8, 1984, for non-medical reasons might not qualify for exemption.
- Lastly, don't send in the form without copying it for your records. Keeping a copy helps track the application’s progress and resolve any issues that might arise.
Misconceptions
Regarding the MV-402 form used in Pennsylvania for applying for a sun screening certificate of exemption, there are several common misconceptions that may confuse applicants. This clarification aims to rectify these misunderstandings.
- Misconception 1:
Any type of tinted windows can get an exemption. In reality, the exemption specifically applies to after-market sun screening products that filter ultraviolet rays, and is primarily intended for medical reasons, allowing only colorless films that filter UV rays.
- Misconception 2:
The exemption applies immediately upon application submission. The truth is, the approval process requires verification of the information provided by both the vehicle owner and a licensed physician or optometrist. The exemption is only valid once officially granted.
- Misconception 3:
The certificate of exemption allows for any level of darkness. This is incorrect, as the exemption is intended for health reasons and is strictly for colorless products that do not significantly darken the windows beyond the legal tinting limits set by state law.
- Misconception 4:
Vehicle owners can self-certify their condition to obtain the exemption. In fact, a licensed physician or optometrist must certify that the vehicle owner (or patient) has a specific medical condition that necessitates the exemption.
- Misconception 5:
The exemption is permanent. The validity of the exemption may be subject to review or renewal requirements, based on state regulations or any changes in the vehicle owner’s medical condition. It's essential for applicants to confirm the duration and conditions of their exemption status.
Understanding these key points can help streamline the application process for a sun screening certificate of exemption and ensure that applicants are fully informed about the requirements and limitations of this accommodation.
Key takeaways
Filling out and using the MV-402 form, which pertains to the application for a sun screening certificate of exemption in the Commonwealth of Pennsylvania, involves several key considerations to ensure that applicants understand the process and requirements. The following takeaways outline the essential aspects of this form:
- Application Purpose: The MV-402 form is specifically designed for individuals or businesses seeking exemption from standard sun screening regulations for their vehicle's windows due to medical reasons or other specific circumstances.
- Required Information: Applicants must provide comprehensive details including full name, PA Driver’s License (PA DL) or Photo ID number for individuals, Business ID for businesses, vehicle information (make, year, VIN, registration plate, title number), and detailed information on the windows requiring sun screening exemption.
- Installation Date Requirement: For the application to be considered, the sun screening must have been installed on the vehicle before September 8, 1984. This requirement underscores the form's focus on vehicles with pre-existing sun screening installations.
- Medical Exemption Documentation: A significant section of the MV-402 form is dedicated to a request for medical exemption, necessitating a licensed physician or optometrist's certification that the applicant requires colorless sun screening products to filter ultraviolet rays for health-related reasons.
- Verification and Certification: The applicant and the certifying physician or optometrist must both sign the form, attesting under penalty of law that all provided information is true and correct. This emphasizes the legal responsibility of both parties to ensure the accuracy of the submitted information.
Understanding these key aspects of the MV-402 form is crucial for applicants seeking a sun screening exemption certificate in Pennsylvania, ensuring that they comply with specific regulatory requirements and accurately represent their need for exemption based on medical necessity or other approved reasons.
Popular PDF Forms
Free Packing Slip Template - It's a critical tool for auditing purposes, providing a clear trail of shipped goods.
Transfer Cna License to South Carolina - Clarifies the eligibility criterion requiring at least 75 hours of training in a state-approved nurse aide I training program.
What Is a Straight Note in Real Estate - Outlines the consequences of defaulting on interest payments, including the acceleration of the entire debt.