Blank Nc Fl2 PDF Template
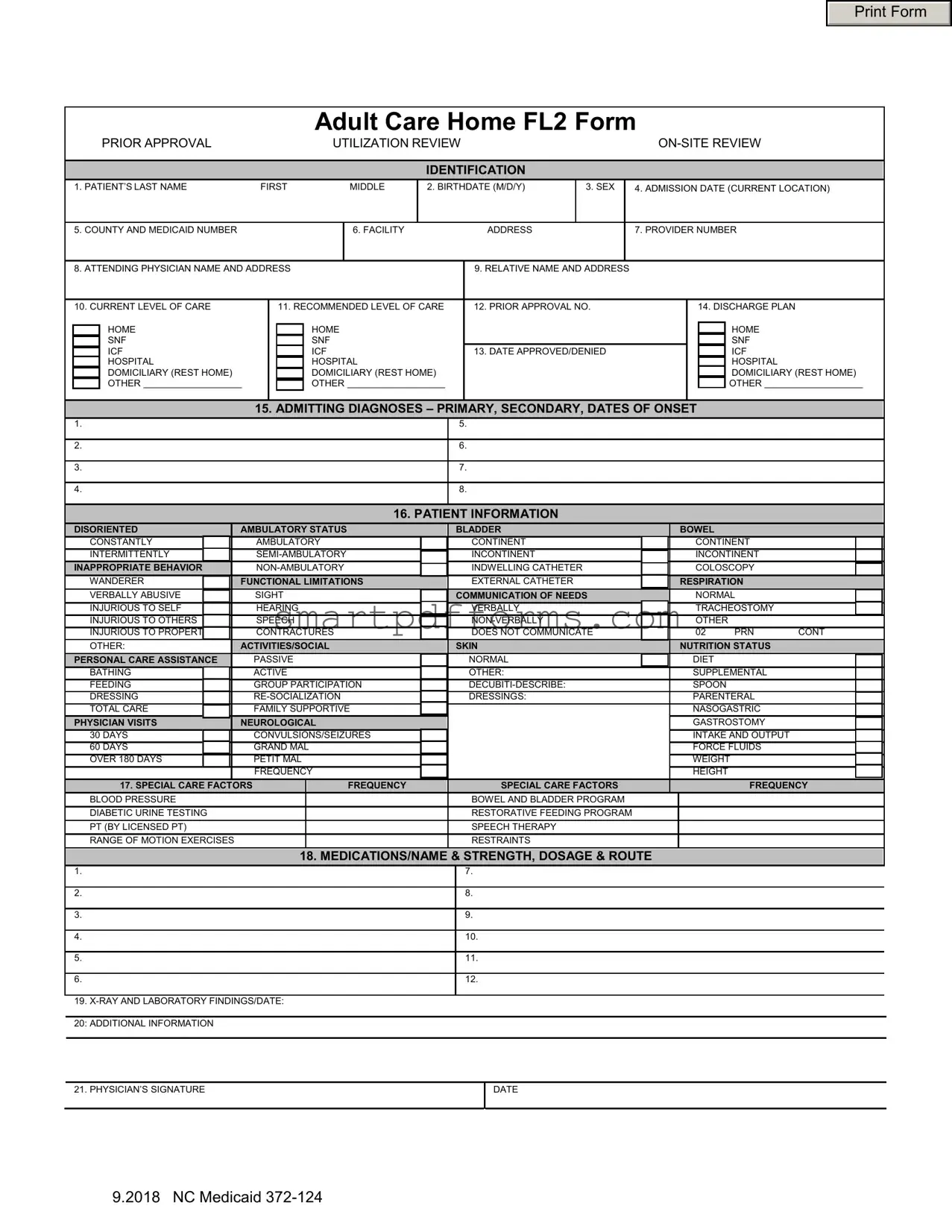
Navigating the landscape of Adult Care Home admissions and ongoing care evaluations can be intricate, as evidenced by the comprehensive details outlined in the North Carolina Adult Care Home FL2 Form. This document is pivotal for health care professionals, patients, and their families, serving as a bridge for communication and ensuring the alignment of care needs with suitable facilities. Covering a wide range of sections, the form captures essential patient information right from basic identification details to the nuanced assessment of current and recommended levels of care. It’s a tool for prior approval, utilization review, and even on-site review processes. The patient's health status, including admission diagnoses, functional limitations, and special care needs, are meticulously documented alongside details of the admitting physician, patient's facility, and the primary contact relative. Medication lists, nutritional needs, and even social engagement capabilities are thoroughly assessed. This form is an essential piece of documentation for managing a patient's transition into, or continuation within, an adult care home setup, ensuring that every facet of their care requirements is appropriately coded and acknowledged for both caregivers and administrative purposes alike.
Preview - Nc Fl2 Form
Print Form
Adult Care Home FL2 Form
|
|
|
PRIOR APPROVAL |
|
|
|
UTILIZATION REVIEW |
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IDENTIFICATION |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
1. PATIENT’S LAST NAME |
FIRST |
MIDDLE |
2. BIRTHDATE (M/D/Y) |
|
3. SEX |
|
4. ADMISSION DATE (CURRENT LOCATION) |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. COUNTY AND MEDICAID NUMBER |
|
|
|
|
|
6. FACILITY |
|
|
ADDRESS |
|
|
7. PROVIDER NUMBER |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
8. ATTENDING PHYSICIAN NAME AND ADDRESS |
|
|
|
9. RELATIVE NAME AND ADDRESS |
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
10. CURRENT LEVEL OF CARE |
|
|
11. RECOMMENDED LEVEL OF CARE |
|
12. PRIOR APPROVAL NO. |
|
|
|
|
14. DISCHARGE PLAN |
|
|
|||||||||||||
|
|
|
HOME |
|
|
|
HOME |
|
|
|
|
|
|
|
|
|
|
|
|
|
HOME |
|
|
||||
|
|
|
SNF |
|
|
|
SNF |
|
|
|
|
|
|
|
|
|
|
|
|
|
SNF |
|
|
||||
|
|
|
ICF |
|
|
|
ICF |
|
|
|
13. DATE APPROVED/DENIED |
|
|
|
|
|
|
ICF |
|
|
|||||||
|
|
|
HOSPITAL |
|
|
|
HOSPITAL |
|
|
|
|
|
|
|
|
|
|
|
|
HOSPITAL |
|
|
|||||
|
|
|
DOMICILIARY (REST HOME) |
|
|
|
DOMICILIARY (REST HOME) |
|
|
|
|
|
|
|
|
|
|
|
DOMICILIARY (REST HOME) |
||||||||
|
|
|
OTHER |
|
|
|
|
OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
15. ADMITTING DIAGNOSES – PRIMARY, SECONDARY, DATES OF ONSET |
|
|
|
|
|||||||||||||||||
|
1. |
|
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
2. |
|
|
|
|
|
|
|
|
|
|
6. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
3. |
|
|
|
|
|
|
|
|
|
|
7. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
4. |
|
|
|
|
|
|
|
|
|
|
8. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
16. PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
DISORIENTED |
|
AMBULATORY STATUS |
|
|
BLADDER |
|
|
|
|
BOWEL |
|
|
|
|
|||||||||||
|
|
CONSTANTLY |
|
AMBULATORY |
|
|
|
CONTINENT |
|
|
|
|
|
CONTINENT |
|
|
|||||||||||
|
|
INTERMITTENTLY |
|
|
|
|
INCONTINENT |
|
|
|
|
|
INCONTINENT |
|
|
||||||||||||
|
|
INAPPROPRIATE BEHAVIOR |
|
|
|
|
INDWELLING CATHETER |
|
|
|
|
|
COLOSCOPY |
|
|
||||||||||||
|
|
WANDERER |
|
FUNCTIONAL LIMITATIONS |
|
|
EXTERNAL CATHETER |
|
|
|
|
RESPIRATION |
|
|
|||||||||||||
|
|
VERBALLY ABUSIVE |
|
SIGHT |
|
|
COMMUNICATION OF NEEDS |
|
|
|
NORMAL |
|
|
||||||||||||||
|
|
INJURIOUS TO SELF |
|
HEARING |
|
|
|
VERBALLY |
|
|
|
|
|
TRACHEOSTOMY |
|
|
|||||||||||
|
|
INJURIOUS TO OTHERS |
|
SPEECH |
|
|
|
|
|
|
|
|
OTHER |
|
|
|
|
||||||||||
|
|
INJURIOUS TO PROPERTY |
|
CONTRACTURES |
|
|
|
DOES NOT COMMUNICATE |
|
02 |
|
PRN |
CONT |
||||||||||||||
|
|
OTHER: |
|
ACTIVITIES/SOCIAL |
|
|
SKIN |
|
|
|
|
NUTRITION STATUS |
|
|
|||||||||||||
|
|
PERSONAL CARE ASSISTANCE |
|
PASSIVE |
|
|
|
NORMAL |
|
|
|
|
|
DIET |
|
|
|
|
|||||||||
|
|
BATHING |
|
ACTIVE |
|
|
|
OTHER: |
|
|
|
|
|
SUPPLEMENTAL |
|
|
|||||||||||
|
|
FEEDING |
|
GROUP PARTICIPATION |
|
|
|
|
|
|
|
SPOON |
|
|
|
|
|||||||||||
|
|
DRESSING |
|
|
|
|
DRESSINGS: |
|
|
|
|
|
PARENTERAL |
|
|
||||||||||||
|
|
TOTAL CARE |
|
FAMILY SUPPORTIVE |
|
|
|
|
|
|
|
|
|
NASOGASTRIC |
|
|
|||||||||||
|
|
PHYSICIAN VISITS |
|
NEUROLOGICAL |
|
|
|
|
|
|
|
|
|
|
GASTROSTOMY |
|
|
||||||||||
|
|
30 DAYS |
|
CONVULSIONS/SEIZURES |
|
|
|
|
|
|
|
|
|
INTAKE AND OUTPUT |
|
|
|||||||||||
|
|
60 DAYS |
|
GRAND MAL |
|
|
|
|
|
|
|
|
|
|
FORCE FLUIDS |
|
|
||||||||||
|
|
OVER 180 DAYS |
|
PETIT MAL |
|
|
|
|
|
|
|
|
|
|
WEIGHT |
|
|
||||||||||
|
|
|
|
|
|
FREQUENCY |
|
|
|
|
|
|
|
|
|
|
HEIGHT |
|
|
|
|
||||||
|
|
|
17. SPECIAL CARE FACTORS |
|
FREQUENCY |
|
|
SPECIAL CARE FACTORS |
|
|
|
|
|
|
FREQUENCY |
||||||||||||
|
|
BLOOD PRESSURE |
|
|
|
|
|
|
|
|
BOWEL AND BLADDER PROGRAM |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
DIABETIC URINE TESTING |
|
|
|
|
|
|
|
|
RESTORATIVE FEEDING PROGRAM |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
PT (BY LICENSED PT) |
|
|
|
|
|
|
|
|
SPEECH THERAPY |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
RANGE OF MOTION EXERCISES |
|
|
|
|
|
|
|
|
RESTRAINTS |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
18. MEDICATIONS/NAME & STRENGTH, DOSAGE & ROUTE |
|
|
|
|
|||||||||||||||
|
1. |
|
|
|
|
|
|
|
|
|
|
7. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
2. |
|
|
|
|
|
|
|
|
|
|
8. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
3. |
|
|
|
|
|
|
|
|
|
|
9. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
4. |
|
|
|
|
|
|
|
|
|
|
10. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
5. |
|
|
|
|
|
|
|
|
|
|
11. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
6. |
|
|
|
|
|
|
|
|
|
|
12. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
19.
21. PHYSICIAN’S SIGNATURE
DATE
9.2018 NC Medicaid
Form Data
| Fact Name | Detail |
|---|---|
| Form Purpose | The NC FL2 form is used for adults entering care homes, indicating medical necessity and preferred level of care. |
| Required Information | The form includes patient identification, admission details, medical condition, current and recommended care levels, and special care factors. |
| Utilization Review | It serves for prior approval, utilization review, and on-site review to ensure appropriate care and resource use. |
| Content Sections | Sections cover patient data, diagnoses, physical and mental capabilities, care needs, medications, and physician's findings and recommendations. |
| Governing Law | Managed under North Carolina Medicaid regulations, ensuring compliance with state-specific health care standards. |
| Completion Requirement | Must be completed by a qualified healthcare provider to confirm the patient's condition and care needs. |
Instructions on Utilizing Nc Fl2
Once it's time to fill out the FL2 form for an adult care home in North Carolina, you'll need a clear, step-by-step guide to ensure no detail is overlooked. This document is crucial for securing the right care level for residents and ensuring appropriate funding and support. With careful attention and thorough detail, this process ensures the individual’s needs are properly communicated and met. Below, you will find a straightforward approach to completing this form accurately.
- Start by entering the Patient’s Last Name, First Name, and Middle Name in the designated area at the top of the form.
- Record the Birthdate of the patient, ensuring the format is Month/Day/Year.
- Mark the Sex of the patient by checking the appropriate box.
- Fill in the Admission Date to the current location, using the same date format as before.
- Provide the County name and the patient's Medicaid Number.
- Enter the Facility Address, including the street, city, and zip code.
- Add the Provider Number associated with the facility.
- Write the Attending Physician's Name and Address, including street, city, state, and zip code.
- Detail a Relative's Name and Address, following the same format as before for contact purposes.
- For both Current Level of Care and Recommended Level of Care, check the appropriate box that matches the patient's needs.
- Enter the Prior Approval No. if applicable.
- Specify the Discharge Plan by checking the appropriate box.
- Fill in the Date Approved/Denied, if already processed.
- In the section for Admitting Diagnoses, list all primary, secondary diagnoses, and dates of onset.
- Under Patient Information, mark all conditions that apply to the patient's status.
- Document any Special Care Factors, including frequency and type of care or monitoring required.
- List all Medications, including name, strength, dosage, and route of administration.
- Include any relevant X-Ray and Laboratory Findings with dates.
- In the Additional Information section, provide any further details that will support the patient’s care and treatment plan.
- Ensure the Physician’s Signature and Date are placed at the bottom of the form to validate the information provided.
After filling out the form, double-check all entries for accuracy and completeness. Submit it to the designated authority as per the facility's procedures or state guidelines. This careful and comprehensive approach helps ensure that the patient receives proper care tailored to their individual needs and circumstances.
Obtain Answers on Nc Fl2
-
What is the FL2 form used for?
The FL2 form serves various purposes within the realm of medical and long-term care. It acts as a mechanism for obtaining prior approval for Medicaid beneficiaries seeking admission to adult care homes including but not limited to skilled nursing facilities, intermediate care facilities, and domiciliary care homes. It also facilitates utilization and on-site reviews by providing detailed patient information to assess the necessity and appropriateness of the care level recommended.
-
Who needs to complete the FL2 form?
The attending physician, in conjunction with the care facility staff, is responsible for completing the FL2 form. The physician provides medical diagnoses and details regarding the patient's care level needs, while the facility staff might contribute information about the patient's daily living capabilities and the special care services required.
-
Where can one obtain an FL2 form?
The FL2 form is available through North Carolina's Department of Health and Human Services (DHHS), particularly from the Division of Medical Assistance. Facilities and physicians can also access it through the DHHS website or directly from Medicaid offices.
-
What information is required on the FL2 form?
Required information includes patient identification and demographic details, the level of care needed, attending physician's details, diagnoses, information on patient's mobility, communication abilities, behavioral issues, and special care factors such as feeding and medication needs.
- Patient's name, birth date, sex, admission date, and Medicaid number.
- Facility and physician information.
- Current and recommended levels of care.
- Medical diagnoses and special care needs.
-
How is the FL2 form processed?
Once completed, the form must be submitted to the appropriate review authority or Medicaid office for processing. This involves verification of information, assessment of care level appropriateness, and prior approval for Medicaid coverage. The form will be either approved or denied based on the established criteria for the required care level.
-
What happens if there's an error on the form?
Errors or omissions can delay the approval process. In case of errors, the form might be returned to the sender for correction. It's critical to review the form thoroughly before submission to ensure all required information is accurately provided.
-
Is the physician's signature required?
Yes, the FL2 form requires the attending physician's signature to validate the information provided regarding the patient's condition and care needs. The physician’s signature certifies the professional assessment and recommendation for the specified level of care.
-
Can an FL2 form be submitted electronically?
Submission methods can vary by location and specific Medicaid office policies. Some regions may accept electronic submissions, while others may require hard copies. It's advisable to consult the local Medicaid office or the DHHS for guidance on acceptable submission formats.
-
What is the significance of the "Recommended Level of Care" section?
This section is crucial as it outlines the physician's recommendation for the patient's placement within a care facility. It affects the determination process for Medicaid coverage and ensures that the patient receives the appropriate level of support and care tailored to their specific health needs.
-
How often does the FL2 form need to be updated?
The frequency of updates varies by patient condition and regulatory requirements. However, it generally needs to be updated upon significant changes in the patient's health status, care requirements, or annually as part of a review process to ensure continued appropriateness of the specified level of care and Medicaid eligibility.
Common mistakes
When filling out the North Carolina Adult Care Home FL2 Form, which is essential in ensuring appropriate care levels and gaining prior approval for Medicaid beneficiaries, individuals often make mistakes that can result in delays or denial of necessary care. Being precise, thorough, and accurate in completing this form is vital. The following are nine common errors made during this process:
Neglecting to include the patient’s full name or misspelling it – This error can lead to confusion and delays in processing as the identity of the patient becomes ambiguous.
Incorrectly listing or omitting the birthdate – Accurate age information is crucial for determining the appropriate level of care and for identity verification purposes.
Failing to accurately detail the admission date – This date is critical for the review process, impacting the approval for the requested level of care.
Omitting or inaccurately providing the county and Medicaid number – This information is essential for ensuring that the application is processed in the correct jurisdiction and for billing purposes.
Leaving the facility address incomplete – A complete address is necessary to verify the location of care and facilitate necessary communications.
Inaccurate provider number entry – This can lead to processing delays or denials, as it is crucial for billing and verifying the provider’s eligibility to offer care.
Forgetting to include the attending physician's name and address – Physician verification is necessary for confirming the level of care needed and for consultation purposes.
Not specifying or wrongly specifying the recommended level of care – This information guides the approval decision, affecting the patient’s care arrangement and coverage.
Insufficient detail in the admitting diagnoses, including primary and secondary diagnoses and dates of onset – Precise medical information is required to ensure the patient receives the proper level of care.
Avoiding these mistakes is imperative for a smooth approval process and to ensure that the individual in need receives the appropriate level of care in a timely manner. It is advisable to review all entries for accuracy and completeness before submitting the form.
Documents used along the form
When handling the needs of adults requiring care, the North Carolina FL2 form plays a crucial role in determining their level of care and eligibility for certain types of facilities or services. However, completing the FL2 form is often just one step in a broader process that involves multiple documents. Each of these documents serves its unique purpose, ensuring comprehensive care and appropriate placement within the health care system. Here's a look at some of those documents often used alongside the FL2 form:
- Physician's Orders: This document outlines the specific care, medications, and procedures ordered by a physician for the patient. It is critical for creating a care plan.
- Medical Power of Attorney (POA): It designates someone to make health care decisions on behalf of the patient if they are incapable of doing so themselves.
- Advanced Directives: This includes living wills and other directives that outline a patient's wishes regarding medical treatment and interventions.
- Medication Administration Record (MAR): Tracks all medications that a patient takes, ensuring they are administered correctly and on time.
- Individual Service Plan (ISP): For residents in certain facilities, an ISP outlines personal goals and how care providers will help the resident meet those goals.
- Assessment and Evaluation Reports: These documents detail the health and needs assessment conducted by healthcare professionals to determine the most appropriate level of care.
- Benefit Eligibility Documents: They verify the patient's eligibility for Medicaid, Medicare, or other insurance programs that may cover the cost of care.
- Guardianship Documents: If a court has appointed a guardian for the patient, these documents verify the guardian's authority to make decisions on behalf of the patient.
- Discharge Plan: When a patient is ready to leave a facility, a discharge plan outlines the care and services they will need after leaving, including follow-up appointments and home care services.
Together, these documents form a comprehensive framework for managing and providing care to adults who need assistance. While the FL2 form is crucial for determining the right care setting, these additional documents ensure that every aspect of the patient's health and welfare is addressed. It's important for caregivers, family members, and health care providers to understand how these documents work together to support the needs of the patient.
Similar forms
The Nursing Home Assessment (MDS) form is similar to the NC FL2 because it collects comprehensive health and personal information to evaluate the level of care needed for a resident. Both documents assess the individual's physical, psychological, and social needs to determine the appropriate care setting.
Hospital Admission Assessment forms share similarities with the NC FL2, as they both gather detailed patient information upon admission, including medical history, current health status, and proposed care plan. These forms are essential for ensuring continuity of care and appropriate treatment planning.
The Home Health Care Assessment form, like the NC FL2, is used to evaluate a patient's needs at home, capturing information on medical history, current health condition, and the level of assistance required for daily activities. Both documents play a crucial role in determining the necessary care services and interventions.
Medicaid Eligibility Form is similar to the NC FL2 in the context of gathering patient identification, medical condition, and care level information to determine Medicaid eligibility and coverage for long-term care services. These forms ensure that individuals receive the financial support they need for their care.
A Comprehensive Psychiatric Evaluation (CPE) form has parallels with the NC FL2 because it collects detailed patient information, focusing on mental health status, to recommend a care plan. Both documents are fundamental in planning effective care, whether in a mental health setting or a general long-term care facility.
Dos and Don'ts
When filling out the NC FL2 form, a critical document for assessing an individual's need for adult care home services, attention to detail is paramount. Below are key do's and don'ts to ensure the accuracy and completeness of your submission.
- Do verify the patient's information before starting. This includes their full name, Medicaid number, and date of birth. Accuracy in these areas is crucial for proper identification and processing.
- Do consult with the patient's attending physician or healthcare provider to accurately complete the medical diagnosis and care level sections. Their input ensures the recommended care level is appropriate.
- Do provide detailed descriptions for the admitting diagnoses, including primary and secondary conditions, along with their dates of onset. This clarity helps in understanding the patient's medical needs.
- Do pay close attention to the patient's personal and health information section, which covers aspects like ambulatory status, mental orientation, and nutritional needs. These details are critical for determining the necessary level of care.
- Do include any special care factors (e.g., blood pressure monitoring, diabetic urine testing) that could affect the patient's care plan. Mention frequency and specifics to outline the required support accurately.
- Don't rush through filling out the form. Take your time to ensure that every section is completed thoroughly. Incomplete or inaccurate information can delay processing and approval.
- Don't forget to list all medications, including name, strength, dosage, and route. This information is crucial for the care facility to understand and manage the patient's medical needs.
- Don't overlook the importance of signing the form. The physician’s signature validates the information provided and is necessary for the form's acceptance.
By adhering to these guidelines, you can contribute to a smoother, more efficient process that benefits all parties involved, especially the individual requiring care.
Misconceptions
Understanding the North Carolina FL-2 Form, commonly used in adult care home assessments and Medicaid applications, is essential for providers, patients, and their families. However, several misconceptions often lead to confusion about its purpose and how it's used. Let's explore eight common misconceptions about the NC FL-2 form.
- The FL-2 form is only for nursing home admissions: While it's commonly associated with nursing home placements, the NC FL-2 form is also used for admission into adult care homes and other long-term care facilities, not just nursing homes.
- Patients can fill out the form themselves: The FL-2 form must be completed by a qualified healthcare provider, such as a physician, nurse practitioner, or physician's assistant, who is familiar with the patient’s medical condition, not by the patients themselves.
- It only assesses physical health: Although it includes detailed sections on physical health, the form also assesses mental and emotional health, including cognitive status and behaviors, indicating its comprehensive nature.
- No ongoing review is necessary: Contrary to this belief, the form often requires updates and reassessments to ensure that the recommended level of care remains appropriate as the patient's condition changes.
- It's the only document needed for long-term care admissions: While the FL-2 form is a critical component of the process, additional documents, such as a patient’s medical history and consent forms, are also needed for admission into long-term care facilities.
- All sections must be filled for every patient: Some sections of the FL-2 form may not apply to every patient. It's vital for the completing healthcare provider to focus on sections relevant to the patient’s specific care needs, although thoroughness is necessary.
- The form is a one-size-fits-all: Each patient's FL-2 form can look very different, reflecting individual care needs and medical conditions. The form is designed to capture the uniqueness of every patient's health situation.
- It guarantees Medicaid approval: Completing and submitting the NC FL-2 form is part of the Medicaid application process for long-term care but does not guarantee Medicaid will approve the application. Medicaid eligibility is determined by a comprehensive assessment of financial and medical needs.
Clarifying these misconceptions is vital for ensuring individuals and families are well-informed about the NC FL-2 form's role in accessing long-term care services. It's always recommended to consult with a healthcare provider or a legal representative specializing in elder law to navigate these processes effectively.
Key takeaways
Filling out and using the NC FL2 form is an important process for individuals who require admission into an adult care home or need to review their current care level. Knowing the key takeaways of this form can simplify the process and ensure all necessary information is accurately provided. Here are seven key takeaways:
- Accurate Patient Information: Ensure the patient's full name, birth date, sex, and current level of care are filled out precisely. Inaccurate information can delay the approval process.
- Admission and Review Details: It's important to note the admission date to the current location and whether the form is for prior approval, utilization review, or an on-site review. This helps in identifying the purpose of the form submission correctly.
- Two Crucial Numbers: Pay special attention to the Medicaid number and the provider number. These are critical for the form's processing and ensuring that the right facilities and services are billed.
- Physician and Relative Information: The attending physician’s and a relative's name and address must be provided. This information is necessary for any follow-up and to ensure all parties involved are kept informed.
- Recommended Level of Care: Clearly indicate the recommended level of care (e.g., SNF, ICF, or domiciliary). This assessment, typically made by healthcare professionals, guides where the patient will receive the best possible care for their needs.
- Admittance Diagnoses and Patient Information: Be thorough in detailing the primary and secondary diagnoses, including onset dates. Understanding the patient's medical condition is essential for the facility to provide adequate care. Moreover, accurately marking the patient's mobility, behavioral, and nutritional statuses helps in ensuring they receive appropriate and individualized care.
- Special Care Factors and Medications: Listing any special care factors, like blood pressure monitoring or diabetic urine testing, along with complete medication details—names, strengths, dosages, and routes—is crucial for the caregiving facility to meet the patient’s health care needs efficiently and safely.
In conclusion, the NC FL2 form plays a pivotal role in facilitating the care for individuals moving into adult care homes. Taking care to fill out each section accurately and thoroughly ensures that the transition is smooth and that the individual receives the care and attention they need without unnecessary delays.
Popular PDF Forms
Tennessee Title Application Form - Secure your vehicle's legal backbone in Tennessee with the comprehensive and straightforward RV-F1315201 form.
Cms-460 - A means for healthcare providers to ensure direct and timely payments from Medicare for covered services.
How to Fill Out an Application - Candidates can list references, providing contacts that can vouch for their character and work ethic.