Blank Onsite Inspection PDF Template
An onsite inspection form serves as a critical tool in evaluating the condition and functionality of a septic system, throwing light on its various components and their current state. Starting with the collection of preliminary system information, this comprehensive form guides inspectors through a series of key checks, including treatment tanks, absorption systems, and disposal/conveyance systems, with a special lookout for any approved alternative technology components that might require extra scrutiny. Aimed solely for internal use, it begins by gathering essential client and system location details before delving into the specifics of the onsite system’s condition. It records weather conditions, system age, dwelling type, and usage, alongside any commercial activities or intensive hobbies that might impact the system. The document not only seeks to uncover the system’s repair history or problems but also assesses its current occupancy and the presence of any adjunct systems that could affect its performance. Tank inspections focus on material types, structure integrity, and maintenance of treatment tanks, whereas the absorption area assessment looks at the presence of inspection ports, odors, and visible signs of malfunction. The form also evaluates the condition of dosing or pump tanks where applicable, summarizing the overall state of the septic system while highlighting any conditions that require urgent health department reporting. Authorized by the customer and inspected by a professional, this form is a vital step towards ensuring the viability of septic systems, concluded with a disclaimer stressing the inspection's limited scope based on current observations without extending any future performance warranties.
Preview - Onsite Inspection Form
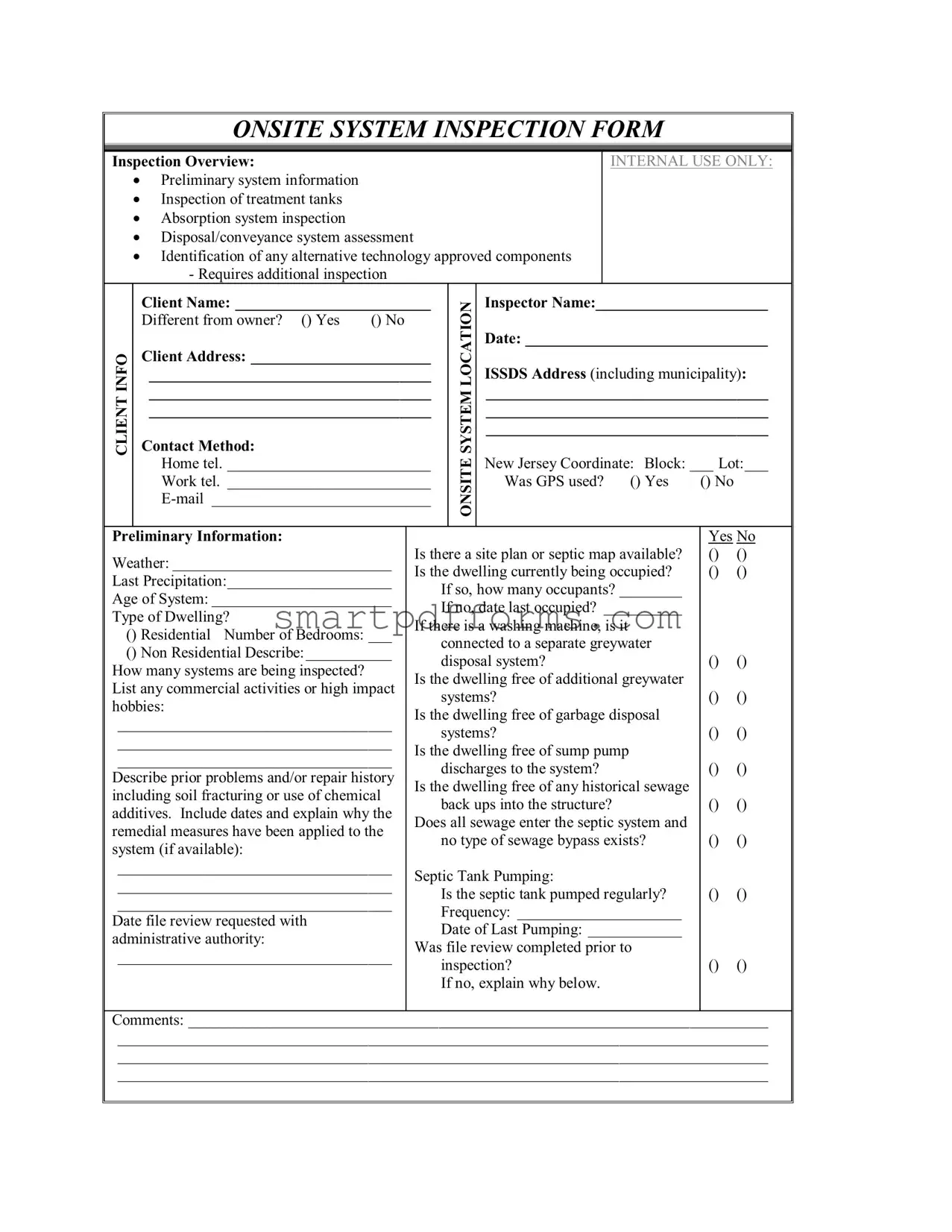
ONSITE SYSTEM INSPECTION FORM
Inspection Overview:
Preliminary system information
Inspection of treatment tanks
Absorption system inspection
Disposal/conveyance system assessment
Identification of any alternative technology approved components
-Requires additional inspection
INTERNAL USE ONLY:
CLIENT INFO
Client Name: _________________________
Different from owner? () Yes () No
Client Address: _______________________
____________________________________
____________________________________
____________________________________
Contact Method:
Home tel. __________________________
Work tel. __________________________
ONSITE SYSTEM LOCATION
Inspector Name:______________________
Date: _______________________________
ISSDS Address (including municipality):
____________________________________
____________________________________
____________________________________
New Jersey Coordinate: Block: ___ Lot:___
Was GPS used? () Yes |
() No |
Preliminary Information:
Weather: ____________________________
Last Precipitation:_____________________
Age of System: _______________________
Type of Dwelling?
() Residential Number of Bedrooms: ___
() Non Residential Describe:___________
How many systems are being inspected? List any commercial activities or high impact hobbies:
___________________________________
___________________________________
___________________________________
Describe prior problems and/or repair history including soil fracturing or use of chemical additives. Include dates and explain why the remedial measures have been applied to the system (if available):
___________________________________
___________________________________
___________________________________
Date file review requested with administrative authority:
___________________________________
Is there a site plan or septic map available? Is the dwelling currently being occupied?
If so, how many occupants? ________
If no, date last occupied? __________
If there is a washing machine, is it connected to a separate greywater disposal system?
Is the dwelling free of additional greywater systems?
Is the dwelling free of garbage disposal systems?
Is the dwelling free of sump pump discharges to the system?
Is the dwelling free of any historical sewage back ups into the structure?
Does all sewage enter the septic system and no type of sewage bypass exists?
Septic Tank Pumping:
Is the septic tank pumped regularly? Frequency: _____________________
Date of Last Pumping: ____________
Was file review completed prior to inspection?
If no, explain why below.
Yes No () ()
() ()
() ()
() ()
() ()
() ()
() ()
() ()
() ()
() ()
Comments: __________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
Treatment Tank: |
|
|
|
|
|
|
Yes |
No |
|
() Septic Tank() Other |
|
Main tank lid opened for inspection? |
|
|
() |
() |
|||
() Greywater |
() |
Liquid level below the tank’s inlet invert? |
|
() |
() |
||||
|
|
|
|
Liquid level below the tank’s outlet invert? |
|
() |
() |
||
Name the material of the system? |
|
Treatment tank pumped for this |
|
|
|
|
|||
() Concrete |
() Block |
|
inspection? |
|
|
() |
() |
||
() Steel |
() Other___________________ |
Are all portions of the tank(s) clear of |
|
|
|
|
|||
|
|
|
|
structures like a deck or a driveway? |
|
() |
() |
||
Approximate treatment tank volume: ______ gal. |
Is the area clear of evidence that sewage |
|
|
|
|||||
|
|
|
|
has surfaced above the treatment tank? |
|
() |
() |
||
Evaluate the conditions of tank below: |
|
Does water flow unimpeded from the |
|
|
|
|
|||
|
|
|
|
treatment tank? |
|
|
() |
() |
|
Satisfactory |
Unsatisfactory |
N/A |
Is an effluent filter a part of the system? |
|
|
() |
() |
||
Top and Lids |
() |
() |
() |
If yes, does it appear properly |
|
|
|
|
|
Inlet Baffle |
() |
() |
() |
maintained? |
|
|
() |
() |
|
Outlet Baffle |
() |
() |
() |
Are there any other types of accessory |
|
|
|
|
|
Cracks or Leaks |
() |
() |
() |
units present? |
|
|
() |
() |
|
Sewage Flow from |
|
|
Depth to top of tank:____________ inches |
|
|
|
|||
Structure |
() |
() |
() |
Depth to top of tank access: ______ inches |
|
|
|
||
|
|
|
|
Comments: ________________________ |
|
|
|
||
|
|
|
|
_________________________________ |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
Absorption Area: |
|
|
|
|
|
|
|
|
|
Name the type of the absorption system? |
|
|
|
|
|
|
|
||
() Disposal Bed |
() Disposal Trench |
|
|
|
|
|
|
||
() Seepage Pit |
() Mounded |
|
|
|
|
|
|
|
|
() Other |
|
|
|
|
|
|
|
|
|
Was the absorption system located? |
() Yes |
() No |
If no, explain below. |
|
|
|
|
||
Are inspection ports present? |
() Yes |
() No |
|
|
|
|
|
||
If yes, how many? _________________________________________________ |
|
|
|
|
|||||
Were the inspection ports checked? |
() Yes* |
() No |
() N/A *All levels observed must be |
|
|||||
included in report |
|
|
|
|
|
|
|
|
|
Was a separate probe dug in the absorption area to confirm the observations in the inspection ports? |
|
||||||||
|
|
|
|
|
() Yes |
() No |
() N/A |
||
Is the area of the absorption system free of sewage odors? |
() Yes |
() No |
|
|
|||||
Does sewage flow from the treatment tank to the absorption system without flowing back? |
|
|
|
|
|||||
|
|
|
|
|
() Yes |
() No |
|
|
|
Is the area above or near any of the system components free from visible signs of effluent or sewage? |
|
||||||||
|
|
|
|
|
() Yes |
() No |
|
|
|
Are the areas at or near the inlet invert of any absorption area component free of visible signs of sewage or
effluent? |
() Yes |
() No |
Are areas above or near system components free of lush vegetation? |
() Yes |
() No |
If exposed, is the distribution box in satisfactory condition? |
() Yes |
() No () N/A |
If not exposed, explain why not: ______________________________________________________
Is the area directly over any part of the absorption system free of any evidence of, large objects (cars, pools,
etc.)?() Yes () No () N/A
Comments: __________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
Sketch the approximate system location in this space provided:
|
Dosing or Pump Tank: |
|
Yes |
No |
N/A |
|
|
|
Does the system contain a pump tank? |
() |
() |
() |
|
|
|
|
Is the pump operating? |
|
() |
() |
() |
|
|
|
Do the alarm(s) on the pump work? |
() |
() |
() |
|
|
|
|
Is the pump elevated above the tank floor? |
() |
() |
() |
|
|
|
|
Is the lid in satisfactory condition? |
() |
() |
() |
|
|
|
|
Is the tank in satisfactory condition? |
() |
() |
() |
|
|
|
|
Is the tank free of accumulated solids? |
() |
() |
() |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Summary: |
Satisfactory |
Satisfactory |
Unsatisfactory |
Requires Additional |
N/A |
|
|
|
|
with Concerns |
|
Investigation |
|
|
|
Condition of the treatment |
|
|
|
|
|
|
|
tank(s) |
() |
() |
() |
() |
() |
|
|
Condition of the conveyance |
|
|
|
|
|
|
|
and pump system(s) |
() |
() |
() |
() |
() |
|
|
Condition of the absorption |
|
|
|
|
|
|
|
area(s) |
() |
() |
() |
() |
() |
|
|
Condition of any accessory |
|
|
|
|
|
|
|
components |
() |
() |
() |
() |
() |
|
Comments: __________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
Health Department Reporting:
Note if any of the following conditions were observed during the inspection:
() 1. Ponding or breakout of sewage or effluent onto the surface of the ground
() 2. Seepage of sewage or effluent into portions of buildings below ground
() 3. Backup of sewage into the building served which is not caused by a physical blockage of the internal plumbing
() 4. Any manner of leakage observed from or into septic tanks, connecting pipes, distribution boxes and other components that are not designed to emit sewage or effluent
Pursuant to N.J.A.C.
If encountered, describe all observed noncompliant conditions encountered during this inspection:
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
Customer Authorization:
I authorize “The Company” to enter the above listed property for the purpose of performing a
Customer signature: _____________________ |
Printed name: |
_____________________________ |
Inspector’s signature: ____________________ |
Printed name: |
_____________________________ |
Disclaimer:
Based on today’s observations and the information provided by the owner(s) or their agent, “The Company” submits this
This form was developed as a cooperative effort of:
Pennsylvania/New Jersey Sewage Management Association;
Rutgers Cooperative Extension New Jersey Agricultural Experiment Station; and
The New Jersey Department of Environmental Protection Septic System Inspection Protocol Subcommittee
Form Data
| Fact Number | Fact Name | Fact Detail | Governing Law(s) |
|---|---|---|---|
| 1 | Inspection Overview | Involves preliminary system information, inspection of treatment tanks, absorption system inspection, disposal/conveyance system assessment, and checking for alternative technology approved components. | N/A |
| 2 | Client Information | Includes client name, whether they are different from the owner, their address, and their contact methods (home phone, work phone, email). | N/A |
| 3 | Onsite System Location | Captures the inspector's name, date of inspection, the address of the Individual Subsurface Sewage Disposal Systems (ISSDS), including municipality and New Jersey Coordinate (Block and Lot), and whether GPS was used. | N/A |
| 4 | Preliminary Information | Gathers information on weather, last precipitation, system's age, dwelling type, number of bedrooms, number of systems inspected, commercial activities/high impact hobbies, prior problems/repairs, whether there's a site plan or septic map, occupancy info, and details on greywater and waste disposal systems. | N/A |
| 5 | Treatment Tank Inspection | Details the inspection of the septic and other treatment tanks including the main tank lid opening, liquid levels, material of the system, whether the treatment tank was pumped for this inspection, condition assessments, and other specific evaluations. | N/A |
| 6 | Absorption Area Inspection | Encompasses the type of absorption system, its location, inspection ports presence and check, position of sewage flow, condition of system components, and additional comments on the absorption area's condition. | N/A |
| 7 | Dosing or Pump Tank Inspection | Includes whether the system contains a pump tank, pump operation and alarm functionality, pump elevation, and the tank's condition. | N/A |
| 8 | Summary and Health Department Reporting | Provides an overall condition summary and details on health department reporting, including the obligation to report certain conditions following N.J.A.C. 7:9A-3.4 within specified timelines. | N.J.A.C. 7:9A-3.4 |
| 9 | Customer Authorization and Disclaimer | Details about customer authorization for property entry and inspection, alongside a disclaimer clarifying the nature of the inspection findings and their implications. | N.J.A.C. 7:9A-1.1 et seq. |
Instructions on Utilizing Onsite Inspection
After an onsite system inspection is completed, a detailed report needs to be prepared that summarizes the condition and functionality of the system. This includes an assessment of the treatment tanks, absorption system, disposal or conveyance system, and any alternative technology approved components, if applicable. Filling out the Onsite Inspection form thoroughly is crucial for maintaining accurate records and ensuring any necessary follow-up actions are clearly identified. Here’s how to fill it out:
- Start by entering the CLIENT INFO section. Write down the client's name, address, and preferred contact method, including home and work telephone numbers and email.
- In the ONSITE SYSTEM LOCATION section, fill in the inspector's name, date of inspection, and the address of the inspected system, including the New Jersey Coordinate Block and Lot numbers. Specify whether GPS was used.
- Under Preliminary Information, record the weather conditions, last precipitation, age of the system, and type of dwelling. Mention the number of bedrooms, any commercial activities or high impact hobbies, and describe any prior problems or repair history.
- Indicate whether a file review was requested with the administrative authority and if a site plan or septic map is available. Detail the dwelling's occupancy status, including the number of occupants or the last occupied date.
- Answer questions regarding the dwelling’s connection to separate greywater disposal systems, the absence of garbage disposal systems, sump pump discharges, historical sewage backups, and if all sewage enters the septic system without bypasses.
- For Septic Tank Pumping, note the frequency of pumping and the date of the last service. Clarify if a file review was completed prior to the inspection and provide comments as necessary.
- In the Treatment Tank section, record observations on the tank’s condition, material, volume, and whether it was pumped for the inspection. Note the presence and condition of any effluent filters, and record the depth to the top of the tank and tank access.
- Assess the Absorption Area, noting the type, whether inspection ports were present and checked, and if there were any odors or visible signs of effluent or sewage. Comment on the condition of the absorption area and sketch its location on the form.
- Fill in details about the Dosing or Pump Tank if applicable, including the operational status of the pump, condition of the tank, and if the tank is free of accumulated solids.
- Summarize the overall condition of the system in the Summary section, marking parts as satisfactory, unsatisfactory, or requiring additional investigation.
- Complete the Health Department Reporting section by noting any conditions observed during the inspection that must be reported to the local administrative authority.
- Finally, obtain the necessary customer and inspector signatures under Customer Authorization to validate the inspection.
Remember, this filled-out form, alongside a copy of the report, must be provided to the local administrative authority within 10 days of completing the inspection. Completing this form diligently ensures accurate documentation, aiding in the overall assessment and maintenance of the onsite sewage disposal system.
Obtain Answers on Onsite Inspection
-
What is the purpose of the Onsite System Inspection Form?
The Onsite System Inspection Form is used for inspecting and assessing various components of a property's onsite sewage disposal system. This includes checking the preliminary system information, treatment tanks, absorption system, disposal/conveyance system, and identifying any approved alternative technology components. This comprehensive inspection helps in understanding the current condition of the sewage system and determining any necessary actions to ensure proper functioning.
-
Who needs to fill out this form?
This form is mainly for internal use by inspectors conducting an onsite sewage disposal system inspection. However, information from the client (property owner or representative) is required, such as their name, address, and preferred contact method. The inspector fills out the detailed aspects of the inspection and the system’s condition based on their observations.
-
What information about the client is required on the form?
The form requires the client's name, address, and how they prefer to be contacted (home telephone, work telephone, and email). Additionally, it asks whether the client's name differs from the property owner’s name.
-
What are the key components inspected as per the form?
The primary components inspected include:
- Preliminary system information
- Treatment tanks inspection
- Absorption system inspection
- Disposal/conveyance system assessment
- Identification of any alternative technology approved components
This thorough inspection helps in identifying any issues that may affect the system's performance.
-
What details are required for the onsite system location?
Information needed for the onsite system location includes the inspector’s name, inspection date, the address of the individual sewage disposal system site (including municipality), and New Jersey Block and Lot coordinates. It also inquires whether GPS was used for location purposes.
-
How does the weather and system’s age impact the inspection?
Recording the weather conditions and the last precipitation can help in understanding the system's current operating conditions, while knowing the age of the system provides insights into potential issues that may be due to wear or outdated components. This information is crucial for a comprehensive evaluation of the system's health.
-
What constitutes a satisfactory inspection result?
Satisfactory inspection results indicate that the treatment tank(s), conveyance and pump system(s), absorption area(s), and any accessory components are in good working condition without any observed issues demanding immediate attention. No ponding, seepage, backup of sewage, or leakage should be observed for a result to be considered satisfactory.
-
What happens if a condition requiring reporting is observed during the inspection?
If a condition that requires reporting is observed, such as ponding or breakout of sewage, seepage into buildings, backup of sewage not caused by physical blockage, or leakage from system components, the inspector must report these findings to the local administrative authority within 24 hours. Moreover, regardless of the observations, a copy of the report must be provided to the local administrative authority within 10 days of report issuance, ensuring compliance with regulations and taking necessary actions to address these issues.
Common mistakes
Filling out an Onsite Inspection form correctly is crucial in ensuring a comprehensive evaluation of a sewage disposal system. Common mistakes can lead to incomplete inspections or inaccuracies in reporting. Here are seven common errors individuals often make when completing an Onsite Inspection form:
Not verifying whether the client information matches the property owner's details can lead to confusion about the system's history and maintenance.
Omitting the use of GPS data for the ISSDS (Individual Subsurface Sewage Disposal Systems) address might result in inaccuracies in identifying the system's exact location, especially in rural areas.
Failing to provide a complete history of the system, including previous problems, repairs, and maintenance activities, can obscure potential issues affecting system performance.
Overlooking the details about the dwelling (such as the number of bedrooms, occupancy status, and high-impact hobbies) may lead to an incorrect assessment of the system's capacity and usage.
Assuming all sewage enters the septic system without confirming no bypass exists might result in overlooking alternative sewage routes contributing to system failures.
Not indicating the date of last pumping or the regularity of septic tank pumping neglects an essential aspect of system maintenance, impacting the inspection's outcome.
Incorrectly assessing or failing to note observations regarding the absorption area, such as the presence of sewage odors or visible effluent, can miss signs of system failure or overloading.
When completing the form, attention to detail and a thorough examination of each component are essential to provide an accurate assessment. Common oversights include:
Ignoring inspection ports: Not checking or incorrectly recording observations from inspection ports can miss critical data about the absorption system's condition.
Neglecting to sketch the system: Failing to provide a diagram of the system's layout can lead to misunderstandings about its configuration and potential problem areas.
Omitting client authorization details: Not securing proper authorization can question the inspection's validity and the inspector's right to access the property.
Ensuring each section of the form is accurately completed with precise and comprehensive data is crucial for a successful onsite system inspection. Avoiding these common mistakes can significantly improve the quality and reliability of the inspection report.
Documents used along the form
In addition to the Onsite Inspection Form, which serves as a comprehensive tool for inspecting sub-surface sewage disposal systems, several other forms and documents often accompany or are utilized in tandem during the inspection process or its preparation. The documents play crucial roles in ensuring a thorough review and compliance with regulatory standards.
- Property Transfer Form: This document is used when ownership of a property is changing hands. It often requires information about the sewage system and proof of inspection to ensure the new owner is aware of the system's status.
- Permit Application: Prior to installation, modification, or repair of a sewage disposal system, a permit might be required. This document is submitted to a local or state regulatory authority and includes details about the proposed work.
- Site Plan: A detailed drawing which provides an aerial view of the entire property, including the location of the septic system components, buildings, wells, and any significant landscape features that could affect the system.
- Maintenance Records: These documents are records of any repairs, pumping, inspection, and general maintenance performed on the septic system. They provide a history of the system's condition and operations.
- Installation Records: Official documentation or receipts that provide information about the septic system’s components, design, and date of installation. These are crucial for understanding the system's capacity and intended function.
- Soil Test Reports: Soil percolation tests and other soil analysis documents are essential in designing a suitable onsite sewage disposal system. They help determine the rate at which soil can absorb water, affecting system design.
- Repair and Alteration Permits: When changes are made to an existing septic system, these permits document what modifications were approved and carried out, ensuring they meet current standards.
- Complaint Forms: If there were issues or complaints lodged against the functioning of the septic system, these forms would contain details and findings related to those complaints.
- Health Department Inspection Reports: Reports from local health departments following their inspections. These may include approvals, recommendations, or requirements for corrections to ensure public health safety.
These documents collectively provide a comprehensive portrayal of the septic system’s design, history, and current condition. They supply valuable information for property owners, inspectors, and regulatory bodies to make informed decisions regarding the operation, maintenance, and compliance of onsite sewage disposal systems.
Similar forms
The Property Inspection Report shares commonalities with the Onsite System Inspection Form, particularly in the structured approach to evaluating and documenting the condition of specific components of a property. Similar to how the Onsite Inspection Form assesses systems like septic tanks and absorption areas, a Property Inspection Report systematically reviews the structural integrity, electrical systems, plumbing, and other critical elements of a building or home. Both documents serve as comprehensive assessments to inform owners or potential buyers about the current state of the inspected entity.
The Home Appraisal Form also parallels the Onsite System Inspection Form in its aim to aggregate crucial information that influences decision-making. While the Home Appraisal Form focuses on evaluating a property's market value based on its condition, location, and features, the Onsite Inspection Form zeroes in on the specifics of a property’s wastewater handling system. Both forms culminate in a synthesized report that impacts financial or ownership decisions, emphasizing the significance of accurate and detailed inspections.
Environmental Impact Assessment (EIA) Reports bear similarities to the Onsite System Inspection Form in their focus on detailed analyses, though in the context of potential environmental effects resulting from proposed projects or activities. Like the Onsite Inspection Form, which includes an examination of septic systems to prevent environmental degradation, EIAs comprehensively evaluate how a project might affect environmental factors such as water quality, wildlife, and vegetation. Detailed observations and findings in both documents inform regulatory compliance and protective measures.
The Building Code Compliance Form is another document with a similar purpose to the Onsite System Inspection Form. This form is used by inspectors to document whether a building or its systems comply with local building codes, including safety standards and regulations. Both forms play crucial roles in ensuring public health and safety by adhering to established guidelines. The Onsite Inspection Form, in evaluating components like septic tanks and absorption systems, ensures that waste disposal does not harm the environment or public health, akin to how Building Code Compliance Forms safeguard against structural and design flaws.
Dos and Don'ts
When filling out the Onsite Inspection form, it's important to follow best practices to ensure the accuracy and completeness of the information provided. Here are five things you should and shouldn't do:
Do:- Provide all requested client information accurately. This includes checking if the client is different from the owner and ensuring contact details are current.
- Use GPS coordinates if available, to provide precise onsite system location details including the New Jersey Coordinate for block and lot identification.
- Record detailed preliminary information, such as the weather conditions, last precipitation, age of the system, and type of dwelling.
- Mention all commercial activities or high-impact hobbies conducted on the property as they can affect the system's evaluation.
- Ensure all sections of the form are completed, including the summary and health department reporting, to provide a comprehensive overview of the system's condition.
- Leave sections blank if the information is available. If a section does not apply, clearly mark it as "N/A" (Not Applicable).
- Forget to include the inspection date and inspector's name at the beginning of the form for proper identification and record-keeping.
- Omit details about prior problems and repairs. Include dates and explanations for any remedial measures applied to the system.
- Skip the step of requesting a file review with the administrative authority, if necessary, for a thorough evaluation.
- Ignore the customer and inspector signature sections at the end of the form. These signatures are necessary to validate the inspection.
Misconceptions
When it comes to the Onsite Inspection Form, used primarily for assessing the condition of septic systems, there are several common misconceptions that can cause confusion for property owners and potential buyers. Let's clear up some of these misunderstandings:
- Misconception 1: The inspection form is only about the septic tank.
Actually, the form covers much more, including treatment tanks, absorption systems, disposal/conveyance systems, and any alternative technology approved components. It provides a thorough check-up of the entire septic system.
- Misconception 2: The form is universally applicable.
While it might seem that way, the provided form specifically notes its development through a cooperation including organizations in Pennsylvania and New Jersey. Different states or regions may have variations based on local regulations and requirements.
- Misconception 3: GPS details are optional.
As indicated in the form, providing New Jersey Coordinate details, including whether GPS was used, is part of the form's requirements. This information helps accurately locate the system for any future reference or inspection needs.
- Misconception 4: It's merely a checklist.
The form actually requires detailed observations, measurements, and conditions of various parts of the system. It goes beyond just ticking boxes; inspectors must provide comments, note conditions, and even sketch system locations.
- Misconception 5: Homeowners can’t understand it.
While it's detailed, the form is structured to be accessible for homeowners to understand the condition and any potential issues with their septic system, as long as they take the time to read through the findings.
- Misconception 6: It doesn’t cover the system’s history.
Previous problems, repairs, and maintenance history are part of the inspection, highlighting the system's performance over time and any recurring issues.
- Misconception 7: Any septic inspector can complete it.
The form requires insights and observations that come from experienced professionals. Inspectors usually have specific training and qualifications, especially in states with stringent septic system regulations.
- Misconception 8: The inspection results are conclusive.
The disclaimer at the end of the form clarifies that while it provides a snapshot of the system’s condition at the time of inspection, it does not guarantee the system’s proper function indefinitely. Various factors like usage, soil type, and maintenance impact the system's operation over time.
Understanding the onsite inspection form is crucial for homeowners and buyers alike. It informs them not just about the current state of the septic system, but also about the property’s overall sanitation and maintenance requirements, debunking these misconceptions is a step toward better, informed decisions regarding property management and transactions.
Key takeaways
Filling out and using the Onsite Inspection form requires attention to detail and adherence to specific procedures. Here are six key takeaways:
- It's crucial to provide comprehensive client and property information, including client name, address, and the specific location of the inspection. Details such as whether the client is the property owner and contact preferences are also vital.
- The form demands meticulous record-keeping of preliminary information, such as weather conditions, last precipitation, and the age of the system being inspected. This establishes the context in which the inspection occurs.
- Accurate documentation of the system's components is required, from treatment tanks to disposal or conveyance systems. This section helps identify the specific areas of the system that need inspection and any required maintenance or repair work.
- Inspectors must assess and report on the condition of the treatment tank, conveyance, and absorption areas, alongside any accessory components. The form provides a structured way to note if these components are satisfactory, unsatisfactory, or require further investigation.
- Any health hazards or noncompliance spotted during the inspection, such as sewage breakouts or leaks, need to be immediately reported to local health departments in accordance with N.J.A.C. 7:9A-3.4 regulations. These measures ensure public health and safety by swiftly addressing potential environmental hazards.
- The inspection is complete only when the customer authorization is signed, granting permission for the inspection and agreeing to the terms laid out by the inspecting company. This part of the form also includes a disclaimer that clarifies the scope of the inspection and any limits on the responsibilities of the inspection company.
Understanding these key points helps inspectors, property owners, and potential property buyers navigate the complexities of onsite system inspections. Proper use of the Onsite Inspection form ensures that inspections are thorough, systems are properly evaluated, and any necessary actions are clearly communicated.
Popular PDF Forms
Super Bill Form - Adaptable for use in a variety of family practice settings, from small clinics to large healthcare facilities.
How to Fill Out Anti Arson Application - Mandates the inclusion of all real estate transactions involving the property in the last three years to check for potential fraud.
If You Give a Statement to the Police Do You Have to Go to Court - A procedural document ensuring the individual's comprehension and voluntary waiver of rights before making a police statement.