Blank Osha 300 PDF Template
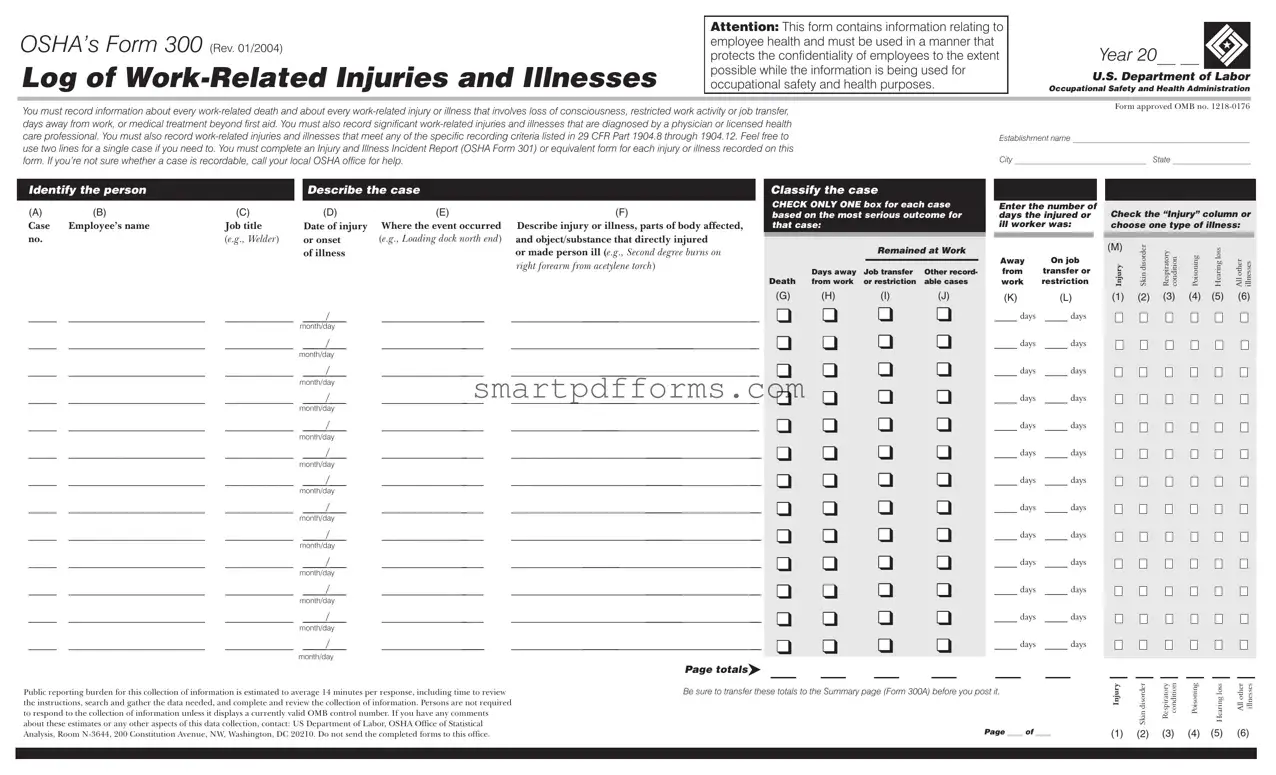
In the landscape of workplace safety and health, the OSHA Form 300 plays a crucial role, serving as a comprehensive Log of Work-Related Injuries and Illnesses. Created with the intent of both documenting and aiding in the prevention of work-related injuries and illnesses, this form is a vital tool for employers. It mandates the recording of every work-related death, injury, or illness that results in loss of consciousness, restricted work activity or job transfer, days away from work, or medical treatment beyond first aid. Additionally, it encompasses the documentation of significant work-related injuries and illnesses diagnosed by a physician or licensed health care professional, as well as those injuries and illnesses that meet specific criteria as outlined in 29 CFR Part 1904.8 through 1904.12. An essential aspect of this process includes filling out an Injury and Illness Incident Report (OSHA Form 301) or an equivalent for each recorded incident, ensuring detailed reporting and analysis. Furthermore, the form necessitates the protection of employee confidentiality to the fullest extent while still utilizing the information for occupational safety and health purposes, representing a balance between transparency and privacy. The significance of the OSHA Form 300 extends beyond mere record-keeping, embodying a systematic approach to identifying, addressing, and ultimately reducing workplace hazards.
Preview - Osha 300 Form
OSHA’s Form 300 (Rev. 01/2004)
Log of
Attention: This form contains information relating to employee health and must be used in a manner that protects the confidentiality of employees to the extent possible while the information is being used for occupational safety and health purposes.
Year 20__ __ 
U.S. Department of Labor
Occupational Safety and Health Administration
You must record information about every
Form approved OMB no.
Establishment name ___________________________________________
City ________________________________ State ___________________
|
|
|
|
|
|
|
|
|
|
|
|
|
Identify the person |
|
|
Describe the case |
|
|
Classify the case |
|
|
|
|
||
|
|
|
|
|
|
|
|
CHECK ONLY ONE box for each case |
|
|
|
|
(A) |
(B) |
(C) |
|
(D) |
(E) |
(F) |
|
|
Enter the number of |
|
Check the “Injury” column or |
|
|
|
|
|
|||||||||
|
|
|
|
|||||||||
|
|
|
|
|||||||||
|
|
based on the most serious outcome for |
|
days the injured or |
|
|||||||
Case |
Employee’s name |
Job title |
|
Date of injury |
Where the event occurred |
Describe injury or illness, parts of body affected, |
|
that case: |
|
ill worker was: |
|
choose one type of illness: |
no. |
(e.g., Welder) |
or onset |
(e.g., Loading dock north end) and object/substance that directly injured |
|
Remained at Work |
|
|
||
|
|
|
|||||||
|
|
of illness |
or made person ill (e.g., Second degree burns on |
|
Away |
On job |
|||
|
|
|
|
|
|
||||
|
|
|
right forearm from acetylene torch) |
|
|
|
|
||
|
|
|
Job transfer |
Other record- |
from |
transfer or |
|||
|
|
|
Days away |
||||||
|
|
|
Death from work |
or restriction |
able cases |
work |
restriction |
||
(M)
Injury
Skindisorder |
Respiratory condition |
Poisoning |
Hearingloss |
Allother illnesses |
_____ |
________________________ |
____________ |
/___ |
__________________ |
__________________________________________________ |
|
|
|
month/day |
|
|
_____ |
________________________ |
____________ |
/___ |
__________________ |
__________________________________________________ |
|
|
|
month/day |
|
|
_____ |
________________________ |
____________ |
/___ |
__________________ |
__________________________________________________ |
|
|
|
month/day |
|
|
_____ |
________________________ |
____________ |
/___ |
__________________ |
__________________________________________________ |
|
|
|
month/day |
|
|
_____ |
________________________ |
____________ |
/___ |
__________________ |
__________________________________________________ |
|
|
|
month/day |
|
|
_____ |
________________________ |
____________ |
/___ |
__________________ |
__________________________________________________ |
|
|
|
month/day |
|
|
_____ |
________________________ |
____________ |
/___ |
__________________ |
__________________________________________________ |
|
|
|
month/day |
|
|
_____ |
________________________ |
____________ |
/___ |
__________________ |
__________________________________________________ |
|
|
|
month/day |
|
|
_____ |
________________________ |
____________ |
/___ |
__________________ |
__________________________________________________ |
|
|
|
month/day |
|
|
_____ |
________________________ |
____________ |
/___ |
__________________ |
__________________________________________________ |
|
|
|
month/day |
|
|
_____ |
________________________ |
____________ |
/___ |
__________________ |
__________________________________________________ |
|
|
|
month/day |
|
|
_____ |
________________________ |
____________ |
/___ |
__________________ |
__________________________________________________ |
|
|
|
month/day |
|
|
_____ |
________________________ |
____________ |
/___ |
__________________ |
__________________________________________________ |
|
|
|
month/day |
|
|
(G) |
(H) |
(I) |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
■■❑ |
(J)
■■❑ ■■❑ ■■❑ ■■❑ ■■❑ ■■❑ ■■❑ ■■❑ ■■❑ ■■❑ ■■❑ ■■❑ ■■❑
(K) |
(L) |
(1) (2) (3) (4) (5) (6) |
||||||||||||
____ days |
____ days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
____ days |
____ days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
____ days |
____ days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
____ days |
____ days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
____ days |
____ days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
____ days |
____ days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
____ days |
____ days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
____ days |
____ days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
____ days |
____ days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
____ days |
____ days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
____ days |
____ days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
____ days |
____ days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
____ days |
____ days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Public reporting burden for this collection of information is estimated to average 14 minutes per response, including time to review the instructions, search and gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have any comments about these estimates or any other aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistical Analysis, Room
Page totals
Be sure to transfer these totals to the Summary page (Form 300A) before you post it.
Page ____ of ____
Injury
(1)
Skindisorder |
Respiratory condition |
Poisoning |
Hearingloss |
Allother illnesses |
|
(2) |
(3) |
(4) |
(5) |
(6) |
|
|
|
|
|
|
|
OSHA’s Form 300A (Rev. 01/2004) |
Year 20__ __ |
|
Summary of |
|
|
Occupational Safety and Health Administration |
||
|
U.S. Department of Labor |
|
|
|
|
|
Form approved OMB no. |
|
All establishments covered by Part 1904 must complete this Summary page, even if no
Using the Log, count the individual entries you made for each category. Then write the totals below, making sure you’ve added the entries from every page of the Log. If you had no cases, write “0.”
Employees, former employees, and their representatives have the right to review the OSHA Form 300 in its entirety. They also have limited access to the OSHA Form 301 or its equivalent. See 29 CFR Part 1904.35, in OSHA’s recordkeeping rule, for further details on the access provisions for these forms.
Number of Cases
Establishment information
Your establishment name __________________________________________
Street |
_____________________________________________________ |
City |
____________________________ State ______ ZIP _________ |
Total number of deaths
__________________
(G)
Total number of cases with days away from work
__________________
(H)
Total number of |
Total number of |
cases with job |
other recordable |
transfer or restriction |
cases |
__________________ |
__________________ |
(I) |
(J) |
Industry description (e.g., Manufacture of motor truck trailers)
_______________________________________________________
Standard Industrial Classification (SIC), if known (e.g., 3715)
____ ____ ____ ____
OR
North American Industrial Classification (NAICS), if known (e.g., 336212)
Number of Days
Total number of days away |
Total number of days of job |
from work |
transfer or restriction |
___________ |
___________ |
____ ____ ____ ____ ____ ____
Employment information (If you don’t have these figures, see the Worksheet on the back of this page to estimate.)
Annual average number of employees |
______________ |
(K)
Injury and Illness Types
Total number of . . .
|
(M) |
|
(1) |
Injuries |
______ |
(2) |
Skin disorders |
______ |
(3) |
Respiratory conditions |
______ |
(L)
(4) |
Poisonings |
______ |
(5) |
Hearing loss |
______ |
(6) |
All other illnesses |
______ |
Total hours worked by all employees last year ______________ |
Sign here
Knowingly falsifying this document may result in a fine.
I certify that I have examined this document and that to the best of my knowledge the entries are true, accurate, and complete.
___________________________________________________________
Company executive |
|
Title |
|
( |
) |
- |
/ / |
Phone |
|
|
Date |
Post this Summary page from February 1 to April 30 of the year following the year covered by the form.
Public reporting burden for this collection of information is estimated to average 58 minutes per response, including time to review the instructions, search and gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have any comments about these estimates or any other aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistical Analysis, Room
OSHA’s Form 301
Injury and Illness Incident Report
Attention: This form contains information relating to employee health and must be used in a manner that protects the confidentiality of employees to the extent possible while the information is being used for occupational safety and health purposes.
U.S. Department of Labor
Occupational Safety and Health Administration
Form approved OMB no.
This Injury and Illness Incident Report is one of the first forms you must fill out when a recordable work- related injury or illness has occurred. Together with the Log of
Within 7 calendar days after you receive information that a recordable
According to Public Law
If you need additional copies of this form, you may photocopy and use as many as you need.
Completed by _______________________________________________________
Title _________________________________________________________________
Phone |
Date _____/ _____ / _____ |
Information about the employee
1)Full name _____________________________________________________________
2)Street ________________________________________________________________
City ______________________________________ State _________ ZIP ___________
3)Date of birth ______ / _____ / ______
4)Date hired ______ / _____ / ______
5) Male
Female
Information about the physician or other health care professional
6) Name of physician or other health care professional __________________________
________________________________________________________________________
7)If treatment was given away from the worksite, where was it given?
Facility _________________________________________________________________
Street _______________________________________________________________
City ______________________________________ State _________ ZIP ___________
8)Was employee treated in an emergency room?
Yes
No
9)Was employee hospitalized overnight as an
Yes
No
Information about the case
10)Case number from the Log _____________________ (Transfer the case number from the Log after you record the case.)
11) |
Date of injury or illness |
______ / _____ / ______ |
|
12) |
Time employee began work ____________________ |
AM / PM |
|
13) |
Time of event |
____________________ |
AM / PM Check if time cannot be determined |
14)What was the employee doing just before the incident occurred? Describe the activity, as well as the tools, equipment, or material the employee was using. Be specific. Examples: “climbing a ladder while carrying roofing materials”; “spraying chlorine from hand sprayer”; “daily computer
15)What happened? Tell us how the injury occurred. Examples: “When ladder slipped on wet floor, worker fell 20 feet”; “Worker was sprayed with chlorine when gasket broke during replacement”; “Worker developed soreness in wrist over time.”
16)What was the injury or illness? Tell us the part of the body that was affected and how it was affected; be more specific than “hurt,” “pain,” or sore.” Examples: “strained back”; “chemical burn, hand”; “carpal tunnel syndrome.”
17)What object or substance directly harmed the employee? Examples: “concrete floor”; “chlorine”; “radial arm saw.” If this question does not apply to the incident, leave it blank.
18) If the employee died, when did death occur? Date of death ______ / _____ / ______
Public reporting burden for this collection of information is estimated to average 22 minutes per response, including time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Persons are not required to respond to the collection of information unless it displays a current valid OMB control number. If you have any comments about this estimate or any other aspects of this data collection, including suggestions for reducing this burden, contact: US Department of Labor, OSHA Office of Statistical Analysis, Room
Form Data
| Fact Number | Fact | Governing Law(s) |
|---|---|---|
| 1 | The OSHA 300 Form is for logging work-related injuries and illnesses. | 29 CFR Part 1904 |
| 2 | It records every work-related death and work-related injury or illness that involves loss of consciousness, restricted work activity or job transfer, days away from work, or medical treatment beyond first aid. | 29 CFR Part 1904.7 |
| 3 | Significant work-related injuries and illnesses that are diagnosed by a physician or licensed health care professional must be recorded. | 29 CFR Part 1904.7 |
| 4 | It also covers the recording of specific work-related injuries and illnesses detailed in 29 CFR Part 1904.8 through 1904.12. | 29 CFR Part 1904.8-1904.12 |
| 5 | For each recorded injury or illness, an Injury and Illness Incident Report (OSHA Form 301) or equivalent form must be completed. | 29 CFR Part 1904.29 |
| 6 | If there's uncertainty about whether a case is recordable, contacting the local OSHA office for assistance is recommended. | N/A |
| 7 | State-specific variations might exist, and compliance with both federal and local regulations is necessary. | Varies by state |
Instructions on Utilizing Osha 300
Filling out the OSHA Form 300, the Log of Work-Related Injuries and Illnesses, is a crucial process for tracking workplace safety incidents. It's designed to record specific details about work-related injuries or illnesses that meet certain criteria, such as days away from work, restricted work, or medical treatment beyond first aid. These precise records help in analyzing workplace safety and health conditions. Below are the steps to properly fill out the form, ensuring every required detail is accurately captured.
- Locate the Year field at the top of the form and enter the four-digit year for which the log is being recorded.
- Write the Establishment’s name, City, State, and Identify the person responsible for record-keeping in the designated areas at the top of the form.
- For each case, start by entering the Employee’s name and Job title in columns (A) and (B).
- Record the Date of injury or onset of illness in column (C), ensuring you use the format month/day.
- Describe Where the event occurred in column (D), providing a specific location for accuracy.
- In column (E), Describe the injury or illness, parts of the body affected, and the object/substance that directly injured or made the person ill with as much detail as possible.
- Check one box in column (F) to Classify the case based on the most serious outcome, such as days away from work, job transfer, or restriction.
- Enter the Number of days the injured or ill worker was away from work or on job transfer or restriction in columns (G) and (H) respectively, if applicable.
- If the case was an Injury, check the corresponding box in column (I). For types of illness, choose the appropriate type in columns (J1) to (J6).
- Remember to use two lines for a single case if you need more space to describe the injury or illness thoroughly.
- Upon completing records for all cases in a year, tally the Page totals at the bottom of the form. This includes counting all incidents and outcomes recorded.
- Finally, ensure all totals are accurately transferred to the Summary page (Form 300A) before posting it as required.
It’s essential to review each entry for completeness and accuracy. If there’s uncertainty about whether a case is recordable, contacting the local OSHA office for guidance can provide clarity. This form plays a vital role in workplace safety management by offering valuable data for preventing future injuries and illnesses.
Obtain Answers on Osha 300
What is OSHA’s Form 300 and why is it important?
OSHA's Form 300, known as the "Log of Work-Related Injuries and Illnesses," serves as a critical record-keeping tool that helps employers track work-related injuries and illnesses that occur in the workplace. Its importance lies in its ability to collect detailed information about every work-related death, injury, or illness that requires medical treatment beyond first aid, results in loss of consciousness, restricted work activity or job transfer, or any days away from work. Additionally, it covers significant work-related injuries and illnesses diagnosed by a physician or licensed health care professional, along with conditions that meet specific recording criteria outlined in 29 CFR Part 1904.8 through 1904.12. This documentation is essential for understanding workplace hazards, improving safety programs, and preventing future incidents, while also ensuring compliance with OSHA regulations.
Who needs to fill out the OSHA Form 300?
All businesses with more than 10 employees that are not classified in certain low-risk industries must complete OSHA's Form 300. It's mandatory for these employers to maintain a log for each establishment or site. The requirement aims at ensuring a thorough record of work-related injuries and illnesses, except for those incidents that involve signs of the common cold or flu. Employers should regularly review and update this log to ensure compliance with OSHA standards and to foster a safer work environment.
How should the information on the OSHA Form 300 be treated concerning employee privacy?
The information on OSHA Form 300 involves sensitive details regarding employee health and must be handled with the utmost confidentiality. While employers are required to document and keep detailed records of work-related injuries and illnesses, it is crucial to protect the privacy of affected employees as much as possible. This means limiting the access to these records to individuals with a legitimate need to know as part of managing occupational safety and health practices. Additionally, if an illness is of a sensitive nature, such that openly disclosing it could violate an employee's privacy, employers are allowed to enter "privacy case" instead of the employee's name. This approach balances the need for workplace safety oversight with the right to confidentiality.
What steps should be taken if there is uncertainty about whether an injury or illness is work-related and recordable on the OSHA Form 300?
If there is any doubt about whether an injury or illness is work-related and meets the criteria for recording on the OSHA Form 300, employers are encouraged to seek clarification. The first step is to review the specific recording criteria outlined in OSHA's 29 CFR Part 1904 regulations thoroughly. If uncertainty remains after reviewing the criteria, employers should contact their local OSHA office for assistance. OSHA provides guidance to help employers determine the work-relatedness and recordability of injuries and illnesses, ensuring that only those cases that truly meet the requirements are documented. This step is essential for maintaining the integrity of the data on work-related injuries and illnesses and for ensuring compliance with OSHA regulations.
Common mistakes
When completing OSHA’s Form 300, commonly known as the Log of Work-Related Injuries and Illnesses, individuals often encounter several common errors. These mistakes can impact the accuracy and integrity of workplace health and safety records. Understanding and avoiding these mistakes is crucial for effective record-keeping and compliance with OSHA regulations.
Not maintaining confidentiality: Given that Form 300 contains sensitive health information, it's imperative to handle and store it in a way that protects employee confidentiality.
Recording non-work-related cases: The form is designated exclusively for work-related injuries and illnesses. Including non-work-related incidents can lead to confusion and inaccuracies.
Incorrect classification of cases: Each case must be classified based on the most serious outcome, such as days away from work or job restriction. Misclassification can skew the data and affect workplace safety evaluations.
Failure to describe the incident clearly: Vague descriptions or omitting details about the injury, the part of the body affected, and how the injury occurred can hinder understanding and prevention efforts.
Omitting cases that require recording: Some injuries or illnesses, especially those requiring medical treatment beyond first aid or involving lost workdays, may inadvertently be left off the form.
Inaccurate tracking of days: Miscounting the number of days away from work or on job transfer/restriction can affect the severity assessment of the incident.
Not completing an Incident Report Form (OSHA Form 301) for each recordable injury or illness: Each recorded injury or illness on Form 300 should have a corresponding detailed report on Form 301, or an equivalent form, which is often overlooked.
Preventing these mistakes requires careful attention to detail, a thorough understanding of OSHA’s record-keeping requirements, and a commitment to accurate and confidential documentation of workplace injuries and illnesses.
Documents used along the form
When handling workplace safety and health management, the OSHA Form 300 plays a pivotal role in recording and analyzing work-related injuries and illnesses. However, to maintain a comprehensive safety program and comply with federal regulations, several other forms and documents are often utilized alongside the OSHA Form 300. These materials serve various purposes, from providing detailed incident reports to summarizing annual data. Understanding each document's purpose can help ensure that a workplace not only complies with OSHA regulations but also fosters a safer environment for all employees.
- OSHA Form 300A - Summary of Work-Related Injuries and Illnesses: This form is a yearly summary of all incidents recorded on the OSHA Form 300. It must be posted in a visible location within the workplace from February 1 to April 30 of the year following the recorded incidents to inform employees about the injuries and illnesses that occurred in the previous year.
- OSHA Form 301 - Injury and Illness Incident Report: For every incident recorded on the OSHA Form 300, a detailed report must be filed using Form 301. This form captures more in-depth information about how the injury or illness occurred, providing a narrative that can help in understanding and preventing future incidents.
- OSHA Form 300 Log - The actual log where work-related injuries and illnesses are recorded. This form requires updates as new incidents occur and serves as a historical record of workplace safety.
- Employee Training Records - Documentation of all safety and health training given to employees. These records are crucial for compliance and for proving that employees have been educated on workplace hazards and safety practices.
- Medical Records - Detailed records of any medical treatment given to employees as a result of work-related injuries or illnesses. These documents are sensitive and must be kept confidential, accessible only by authorized personnel.
- Hazard Assessment Records - Documents detailing the findings of workplace hazard assessments. These assessments help in identifying and mitigating risks that could lead to injuries or illnesses.
- Inspection Reports - Reports from any inspections conducted within the workplace, whether internal or by OSHA inspectors. These reports can provide insight into areas that need improvement or hazards that have been overlooked.
- Incident Investigation Reports - Reports generated after investigating workplace incidents, providing details on the causes and suggesting preventive measures.
- Safety Meeting Minutes - Records of safety meetings held with employees, including topics discussed, concerns raised by employees, and any decisions or action items related to workplace safety.
Utilizing these documents in conjunction with the OSHA Form 300 helps employers create a safer workplace by addressing and mitigating risks, ensuring compliance with safety regulations, and fostering an environment of transparency and continuous improvement. Understanding and effectively managing these forms and documents is essential for any organization committed to the health and safety of its workforce.
Similar forms
OSHA’s Form 301: This document, mentioned within the Form 300 instructions, is an Injury and Illness Incident Report. It complements Form 300 by providing more detailed information about each individual injury or illness recorded. Think of it as a deep dive into the specifics of each case, where you describe how the injury or illness occurred, the nature of the harm, and any factors that contributed to the event.
Form 300A: This is the Summary of Work-Related Injuries and Illnesses. Form 300A takes the totals from Form 300 and displays them in a summary format. It's designed for posting in a visible location within the workplace to communicate the overall safety record of the establishment over the course of a year, making integral safety statistics accessible to employees.
Workers’ Compensation Claims: While not a specific form, workers' compensation claims require similar information to what is recorded on OSHA’s Form 300. These claims also involve details about work-related injuries or illnesses, such as the nature and circumstances of the injury, medical treatment received, and any time off work due to the injury.
FMLA (Family and Medical Leave Act) documentation: For injuries or illnesses that qualify for FMLA leave, the required paperwork often overlaps with the information on OSHA’s Form 300. This includes the dates of absence, medical reasons for the leave, and any relevant medical certification.
Insurance Claims Forms: For work-related injuries or illnesses, insurance claims (whether health, disability, or liability insurance) require detailed information about the incident, much like OSHA’s Form 300. These forms are used to assess the case and determine coverage and benefits.
Incident Investigation Reports: These are internal company reports that are compiled following workplace accidents or incidents. Like the OSHA Form 300, they include comprehensive details about what happened, including who was involved, the injuries or illnesses incurred, and what factors contributed to the incident.
Safety Audit Reports: Safety audits sometimes result in documentation that resembles the OSHA Form 300, particularly in regard to logging hazards, near misses, or safety non-compliances that could potentially lead to injury or illness if not addressed.
Risk Assessment Documentation: Part of preventing workplace injuries and illnesses involves identifying potential risks and documenting them. This pre-emptive form of documentation can resemble the injury and illness logging on Form 300 but focuses on potential rather than actual incidents.
Job Hazard Analysis (JHA) Reports: These reports, which evaluate potential hazards associated with specific job tasks, can mirror the preventive aspect of Form 300's intent. While JHAs aim to mitigate risk before incidents occur, they share the goal of maintaining a safe and healthy workplace.
Occupational Health Surveillance Records: Similar to OSHA’s Form 300, these records keep track of health trends and patterns within a working population to prevent occupational injuries and illnesses. They collect data on the prevalence and incidence of work-related health conditions and the effectiveness of intervention efforts.
Dos and Don'ts
When filling out the OSHA Form 300, it's crucial to pay attention to details and follow the guidelines accurately to ensure compliance and maintain workplace safety. Below are five key things you should do and five things you shouldn't do when completing the form.
Things You Should Do
Ensure that every work-related death, injury, or illness is recorded, especially those requiring medical treatment beyond first aid or resulting in loss of consciousness, restricted work, or job transfer.
Use two lines for a single case if necessary to provide a detailed description of the injury or illness, including the part of body affected and the object or substance that caused the harm.
Classify each case correctly based on the most serious outcome, whether it's days away from work, job transfer, or another recordable case category.
Maintain the confidentiality of employees by handling the information in a manner that protects their privacy to the extent possible while using the data for safety and health purposes.
Complete an Injury and Illness Incident Report (Form 301) for each recorded injury or illness to provide more details about the case.
Things You Shouldn't Do
Don't overlook the importance of accurately identifying each case, including employee's name, job title, and the date and location of the injury or illness onset.
Avoid guessing when it comes to classifying the case; if unsure, seek clarification from your local OSHA office.
Do not ignore the specific recording criteria listed in 29 CFR Part 1904.8 through 1904.12. Ensure each recordable injury and illness meets these requirements.
Refrain from submitting the completed forms to the wrong address. These records should be maintained at your establishment, not sent to the Department of Labor unless specifically requested.
Never falsify records or underreport injuries and illnesses. Accurate reporting is crucial for compliance and for maintaining a safe work environment.
Misconceptions
When it comes to workplace safety, understanding the details about OSHA's Form 300 is crucial. However, there are a few common misconceptions that often lead to confusion. Here are four of those misconceptions clarified:
- Misconception 1: All Work-Related Injuries and Illnesses Must Be Recorded
This isn't entirely true. While you must record many types of work-related injuries and illnesses, there are specific criteria that must be met for an incident to be recordable. For example, injuries that only require first aid and do not involve time away from work, job restrictions, or medical treatment beyond first aid are not typically recorded.
- Misconception 2: You Must Send the Completed OSHA 300 Form to OSHA Annually
Actually, the OSHA 300 Log and the OSHA Form 300A Summary must be maintained in the workplace, but they are not sent to OSHA annually. These records must be retained in the workplace for five years following the end of the calendar year that these records cover. However, certain data from the Form 300A must be submitted electronically if your establishment is covered by these requirements.
- Misconception 3: Small Employers Are Exempt from Keeping OSHA 300 Logs
While it's true that employers with ten or fewer employees at all times during the last calendar year do not have to keep OSHA 300 Logs, there are exceptions. Certain industries identified by OSHA as high hazard are required to maintain these records regardless of the number of employees. It’s essential to check whether your business falls under these exceptions.
- Misconception 4: Only Full-Time Employee Injuries and Illnesses Should Be Recorded
This is not correct. OSHA's recording requirements apply to all employees on your payroll, whether they are full-time, part-time, seasonal, or temporary workers. Additionally, it also includes injuries and illnesses to workers who are not on your payroll if you supervise these workers on a day-to-day basis.
Understanding these misconceptions can greatly help in maintaining an accurate and compliant record-keeping process. This not only ensures the safety and health of employees but also ensures that your company is meeting federal requirements. Always remember, when in doubt, refer to the detailed guidelines provided by OSHA or seek professional advice.
Key takeaways
Understanding how to correctly fill out and use OSHA's Form 300 is crucial for maintaining a safe and legally compliant workplace. Here are seven key takeaways that can help employers manage this important responsibility:
- Confidentiality is key. The Form 300 contains sensitive information about employees' health and injuries. It's imperative to handle and store this form in a way that respects and protects employee confidentiality at all times.
- Record a wide range of incidents. Not only should deaths and serious injuries be recorded, but also incidents resulting in lost work days, restricted work, job transfers, or medical treatment beyond first aid. Also, anything diagnosed by a physician or licensed health professional needs to be included.
- Use clear, descriptive language. When describing an injury or illness, clarity is critical. Include specific details like the part of the body affected and how the injury or illness occurred, ensuring the description can be understood without assuming specialized knowledge.
- Classification matters. Correctly classifying a case as either an injury or an illness, based on the most serious outcome, is essential. Whether an incident led to death, days away from work, job restriction, or a transfer, it should be classified accurately to ensure proper handling and record-keeping.
- Don’t forget the Form 301. For each entry on the Form 300, a detailed Incident Report (OSHA Form 301 or an equivalent) must be completed. This step is crucial for documentation purposes and provides a more complete picture of each incident.
- Accuracy is non-negotiable. The number of days away from work or on job restriction must be counted accurately. This includes being mindful of recording the exact numbers on the form to help with statistical analysis and future preventive measures.
- Adherence to deadlines and updates. Updating the log with any new information about each case or correcting inaccuracies is an ongoing responsibility. Additionally, transferring totals to the Summary page (Form 300A) before the posting deadline is critical for compliance.
By meticulously following these guidelines, employers can not only comply with OSHA regulations but also foster a culture of safety and transparency in the workplace. Remember, a well-maintained OSHA Form 300 can be a tool not just for compliance, but for analyzing and preventing future injuries and illnesses.
Popular PDF Forms
Tn Counter Offer - Facilitates clear, legally sound negotiations between parties in a Tennessee real estate transaction by providing a structured format for counteroffers.
Ohio Repossession Laws - Provides space for the repossession agency's information, ensuring that all parties involved in the repossession are properly notified and authorized.
Ps3971 - Training on how to complete the PS 3971 is provided to USPS employees as part of their orientation.