Blank Return Work Medical Certification PDF Template
Ensuring a smooth transition back to work for employees after a medical leave is crucial for maintaining workplace efficiency and supporting employee health. The Return to Work Medical Certification form plays a pivotal role in this process. It bridges the gap between medical advice and job requirements, serving both employers and employees. Designed to be filled out in two sections, the form requires input from the employer regarding the employee’s position and contact information, followed by detailed medical certification from a health care provider. This certification assesses the employee's ability to resume work, possibly under specific conditions due to the serious health condition that prompted the leave. Notably, the form adheres to the Genetic Information Nondiscrimination Act of 2008 (GINA), emphasizing the protection of the employee's genetic information by limiting the health data requested. With sections dedicated to outlining any work restrictions and the duration thereof, the form ensures that the return to work is handled with clear communication of the employee's capabilities, safeguarding both the employee's health and the employer's operational requirements.
Preview - Return Work Medical Certification Form
Print Form
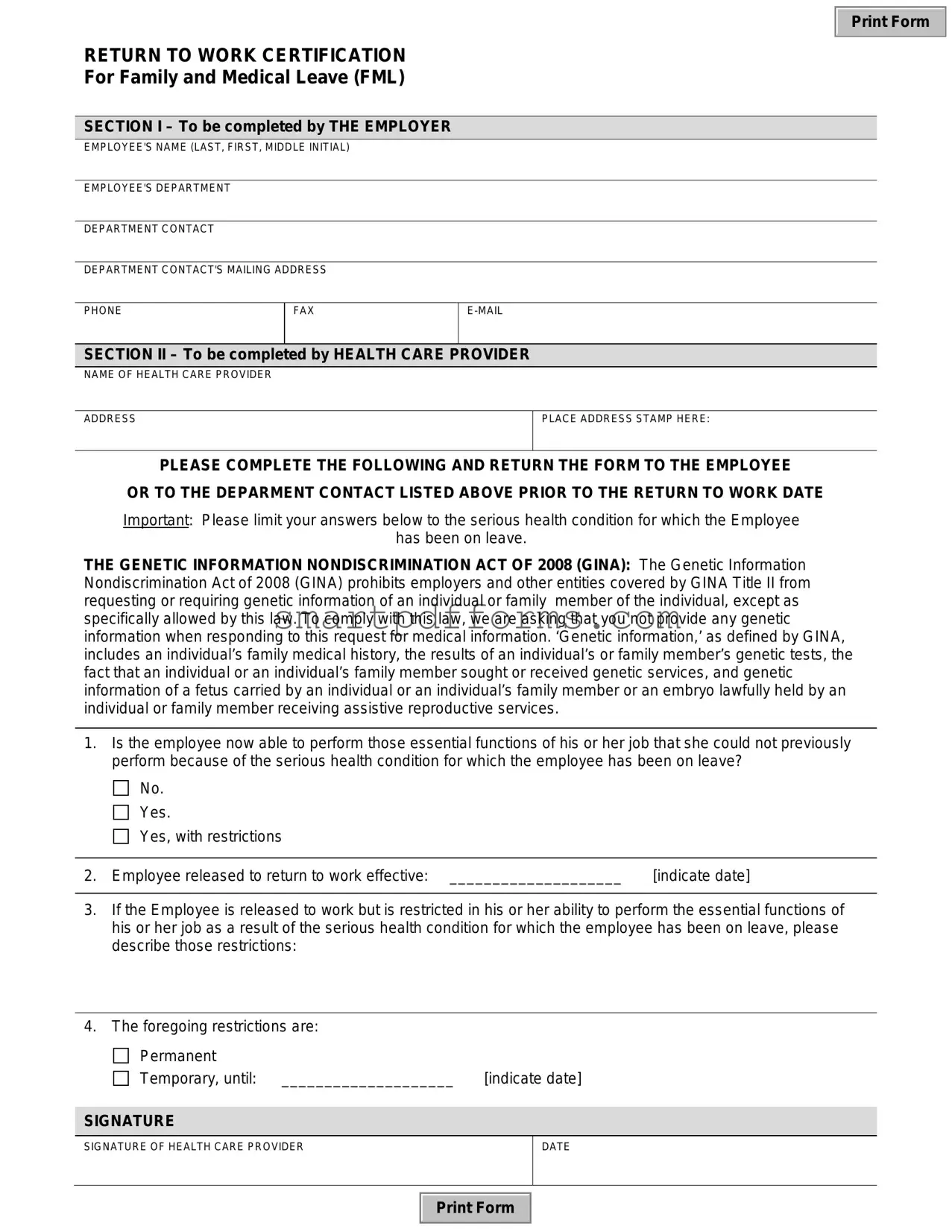
RETURN TO WORK CERTIFICATION
For Family and Medical Leave (FML)
SECTION I – To be completed by THE EMPLOYER
EMPLOYEE'S NAME (LAST, FIRST, MIDDLE INITIAL)
EMPLOYEE'S DEPARTMENT
DEPARTMENT CONTACT
DEPARTMENT CONTACT'S MAILING ADDRESS
PHONE
FAX
SECTION II – To be completed by HEALTH CARE PROVIDER
NAME OF HEALTH CARE PROVIDER
ADDRESS
PLACE ADDRESS STAMP HERE:
PLEASE COMPLETE THE FOLLOWING AND RETURN THE FORM TO THE EMPLOYEE
OR TO THE DEPARMENT CONTACT LISTED ABOVE PRIOR TO THE RETURN TO WORK DATE
Important: Please limit your answers below to the serious health condition for which the Employee
has been on leave.
THE GENETIC INFORMATION NONDISCRIMINATION ACT OF 2008 (GINA): The Genetic Information Nondiscrimination Act of 2008 (GINA) prohibits employers and other entities covered by GINA Title II from requesting or requiring genetic information of an individual or family member of the individual, except as specifically allowed by this law. To comply with this law, we are asking that you not provide any genetic information when responding to this request for medical information. ‘Genetic information,’ as defined by GINA, includes an individual’s family medical history, the results of an individual’s or family member’s genetic tests, the fact that an individual or an individual’s family member sought or received genetic services, and genetic information of a fetus carried by an individual or an individual’s family member or an embryo lawfully held by an individual or family member receiving assistive reproductive services.
1.Is the employee now able to perform those essential functions of his or her job that she could not previously perform because of the serious health condition for which the employee has been on leave?

 No.
No.

 Yes.
Yes.

 Yes, with restrictions
Yes, with restrictions
2. Employee released to return to work effective: ____________________ |
[indicate date] |
3.If the Employee is released to work but is restricted in his or her ability to perform the essential functions of his or her job as a result of the serious health condition for which the employee has been on leave, please describe those restrictions:
4.The foregoing restrictions are:
Permanent |
|
Temporary, until: ____________________ |
[indicate date] |
SIGNATURE
SIGNATURE OF HEALTH CARE PROVIDER
DATE
Print Form
Form Data
| Fact Name | Description |
|---|---|
| Purpose of the Form | This form is used to certify that an employee is able to return to work after taking Family and Medical Leave (FML) due to a serious health condition. |
| Section I Completion | The employer is responsible for completing the first section of the form, which includes details about the employee and the department. |
| Section II Completion | The health care provider must fill out the second section, providing information about the employee's ability to return to work and any limitations. |
| GINA Compliance | The form mentions the Genetic Information Nondiscrimination Act of 2008 (GINA), advising health care providers to exclude genetic information when completing the form. |
| Work Restrictions | If the employee is able to return to work with restrictions, these must be clearly described in the form by the health care provider. |
| Governing Law | The form adheres to the requirements set forth by the Family and Medical Leave Act (FMLA) as well as the Genetic Information Nondiscrimination Act of 2008 (GINA). |
Instructions on Utilizing Return Work Medical Certification
Filling out a Return to Work Medical Certification form is an essential step for employees transitioning back to work after a medical leave, ensuring their readiness to resume their duties without compromising their health. The form requires information from both the employer and the healthcare provider to certify the employee’s ability to return to work, taking into account any necessary restrictions or accommodations. Below are step-by-step instructions to complete this form correctly.
- Section I – To be Completed by The Employer:
- Enter the employee’s full name (last, first, middle initial) in the designated space.
- Fill in the employee’s department to ensure the form is routed correctly.
- Provide the name and contact details (mailing address, phone, fax, and email) of the department contact responsible for managing the employee’s return.
- Section II – To be Completed by Health Care Provider:
- The health care provider must enter their name and address in the space provided. If available, an address stamp can be used for convenience.
- Answer the question regarding the employee’s ability to perform the essential functions of their job that they were unable to perform due to their health condition. Check the appropriate box: No, Yes, or Yes, with restrictions.
- If the employee is cleared to return to work, indicate the effective date of return.
- Describe any restrictions the employee has if they are unable to fully perform their job duties. This includes limitations or necessary accommodations.
- Specify if the restrictions are Permanent or Temporary. If temporary, provide an end date for these restrictions.
- The health care provider must sign and date the form to validate the certification.
Once both sections are completed, the form should be returned to the designated department contact as indicated in Section I. This ensures the employee’s return to work is managed appropriately, respecting any limitations or accommodations specified by the health care provider. It's important for both the employer and the employee to keep a copy of this form for their records. Collaborating closely with healthcare providers, employees, and employers can facilitate a smooth and safe transition back to work for everyone involved.
Obtain Answers on Return Work Medical Certification
Frequently Asked Questions about the Return to Work Medical Certification Form
-
What is the purpose of the Return to Work Medical Certification form?
The Return to Work Medical Certification form plays a crucial role in ensuring that an employee who has taken Family and Medical Leave (FML) due to a serious health condition is ready to resume work. This document, completed by the employee's health care provider, communicates the employee's capability to perform their job functions post-leave. It informs the employer whether the employee can return without restrictions or with certain limitations related to their serious health condition.
-
Who needs to complete the Return to Work Medical Certification form?
There are two sections in the Return to Work Medical Certification form: Section I must be filled out by the employer, providing details about the employee and the department contact information. Section II requires completion by the health care provider, where information regarding the employee's ability to resume work and any work restrictions are documented.
-
What information is required from the health care provider in the form?
The health care provider is asked to specify whether the employee is capable of returning to work and performing the essential functions of their job post-leave. If restrictions apply, the provider must detail these limitations. Additionally, the provider will indicate whether these restrictions are permanent or temporary, including the expected duration of such restrictions if temporary.
-
What should not be included in the form due to the Genetic Information Nondiscrimination Act of 2008 (GINA)?
In adherence to GINA, health care providers are instructed not to include any genetic information when completing the form. This includes family medical history, the results of genetic tests, or any services received related to genetic testing. The Act aims to protect individuals from discrimination based on their genetic information.
-
What happens if the employee is unable to return to work without restrictions?
If the employee is deemed unable to resume their job functions without restrictions, the health care provider must clearly outline these limitations on the form. It's then the responsibility of the employer to determine if reasonable accommodations can be made to allow the employee to work within those restrictions.
-
How should the completed form be submitted?
The completed form should be returned either directly to the employee or to the department contact listed in Section I by the health care provider. It's imperative that this is done before the employee's scheduled return to work date to ensure a smooth transition back to work.
-
What are the next steps after the form is submitted?
Once the form is received, employers should review the health care provider’s recommendations and determine if any accommodations are needed for the employee’s return. Communication with the employee is essential to discuss any necessary adjustments or modifications to their work environment or duties to accommodate any restrictions outlined by the health care provider.
Common mistakes
Filling out the Return to Work Medical Certification form is a crucial step in ensuring a smooth transition back to work for employees after a medical leave. However, mistakes can occur during this process, affecting the employee's ability to return to work efficiently and correctly. Let's walk through ten common mistakes made when completing this form:
Missing the employer’s section completion: The initial part of the form is designated for the employer, which includes critical details like the employee's name, department, and contact information. Neglecting this section can lead to confusion and delays.
Not fully completing the health care provider's section: Every part of the health care provider’s section is essential for assessing the employee's readiness to return to work. Incomplete information may result in unnecessary back-and-forth communication.
Not clearly indicating if the employee is able to perform their job functions. The question about the employee's capability to perform essential job functions needs a clear yes, no, or "yes, with restrictions" answer. Ambiguity here can lead to misinterpretations.
Omitting the effective date for the employee's return to work. This date is essential for both planning and documentation purposes.
Providing insufficient details on work restrictions: If the employee has limitations, the form requires explicit details about these restrictions. Vague descriptions can lead to misunderstandings about the employee’s capabilities.
Labeling restrictions inaccurately as "Permanent" or "Temporary". This distinction is crucial for understanding the duration of the employee's limitations and planning accordingly.
Failing to sign the form. The health care provider’s signature verifies the authenticity of the information provided. A missing signature can invalidate the form.
Ignoring the date field: Not dating the form is a common oversight that can lead to questions about the recency and relevance of the medical assessment.
Including genetic information. Given GINA's regulations, providing genetic information can inadvertently lead to legal complications. It’s essential to comply with these guidelines.
Misaddressing the form upon return. Whether it’s to the employee or the department contact, ensuring the form reaches the right hands is fundamental for processing the employee's return to work.
Skipping these common mistakes not only streamlines the process but also ensures compliance with legal standards, ultimately facilitating a better transition back to work for the employee.
Documents used along the form
When an employee is preparing to return to work after a medical leave, several important documents often accompany the Return to Work Medical Certification form. These forms together ensure a smooth transition back to the workplace, addressing health concerns, workplace accommodations, and compliance with legal requirements. Here's a look at some of those key documents.
- Employee’s Leave of Absence Request Form: This form initiates the process for a leave of absence, detailing the reason for the leave and the expected duration. It serves as the starting point for the leave process, to which the Return to Work Medical Certification is the concluding step.
- Family and Medical Leave Act (FMLA) Documentation: If the leave qualifies under FMLA, documentation confirming eligibility and outlining the rights and responsibilities of both the employer and employee is necessary. This legal documentation ensures both parties meet their FMLA obligations.
- Reasonable Accommodation Request Form: If the returning employee requires adjustments to their work environment or schedule to accommodate a medical condition, this form outlines those needs. It is essential for initiating discussions on how to best integrate the employee back into their role.
- Workers’ Compensation Claim Form: In cases where the leave is due to a workplace injury, a worker’s compensation claim form may be used. It documents the injury and the treatment received, and it may involve coordination with workers' compensation insurance.
- Job Description: A current job description helps healthcare providers understand the essential functions of the employee's job. This is crucial when determining any restrictions or accommodations necessary upon the employee’s return.
- Emergency Contact Information: Though not directly related to the medical leave process, ensuring that an employee’s emergency contact information is up to date is a good practice during any significant administrative update.
Together, these documents provide a comprehensive framework that supports employees during their transition back to work. They help in clearly communicating the needs and limitations between employees, healthcare providers, and employers, ensuring a safe and effective return to the workplace.
Similar forms
Family Medical Leave Act (FMLA) Certification: Similar to the Return to Work Medical Certification form, the FMLA Certification is used to certify that an employee is eligible for leave due to a serious health condition that makes them unable to perform their job functions. Both require information from a health care provider about the condition and its impact on the employee's job capabilities.
Disability Benefits Forms: These forms, used to apply for disability benefits, are similar because they also require a health care provider to detail an individual's health condition and how it affects their ability to work. Like the Return to Work form, they may specify whether the condition is temporary or permanent and outline any work restrictions.
Workers' Compensation Claim Forms: Workers' Compensation forms are another set that requires detailed medical information following a work-related injury or illness. They are similar in requiring a health care provider's certification of the injury and an assessment of the employee's ability to return to work, including any limitations.
Reasonable Accommodation Requests under the Americans with Disabilities Act (ADA): Like the Return to Work form, these requests require medical documentation to understand the employee's condition and determine necessary accommodations. Both involve assessing how an employee’s health condition or disability affects their work and what modifications may be needed.
Medical Examination Forms for Employment: These forms are completed as part of pre-employment processes or periodic medical examinations during employment. Similar to the Return to Work Certification, they may require a healthcare provider to certify an employee’s fitness for specific job duties, potentially including any restrictions or accommodations.
Insurance Claim Forms: Used for submitting medical claims to insurance companies, these forms often require detailed medical information similar to the Return to Work Medical Certification. Both types of forms necessitate documentation from health care providers about the nature of the health condition and its impact on the individual’s ability to perform work or daily activities.
Medical Leave of Absence Request Forms for Educational Institutions: Students may need to submit these forms to take a medical leave of absence, similar to workers submitting FMLA documentation. These forms often require health care provider certification of the condition affecting the student's ability to attend classes, mirroring the employer's need to understand an employee's ability to perform work when submitting a Return to Work form.
Dos and Don'ts
When it's time to fill out a Return to Work Medical Certification form, following a structured approach can help ensure the process is smooth and the information provided is accurate. Here are some dos and don'ts to keep in mind:
Do:- Read the entire form before starting. Understanding each section's requirements can help ensure all necessary information is readily available.
- Gather all needed information beforehand. This includes the employee’s medical details, the employer's contact information, and any restrictions recommended by the healthcare provider.
- Be clear and concise in your responses. Only include relevant details related to the serious health condition and the employee's ability to return to work.
- Respect privacy laws. Avoid sharing genetic information or any other details not directly related to the task of completing the form in compliance with laws like GINA.
- Check for accuracy. Verify all the details on the form, including dates and medical information, to ensure they are correct.
- Sign and date the form. An official signature from the healthcare provider is often required to confirm the information’s validity.
- Provide clear instructions regarding any work restrictions. If the employee has limitations, describe these carefully to inform the employer about necessary accommodations.
- Use official stamps or letterhead if required. This can help authenticate the document, making the return-to-work process smoother.
- Communicate directly with the employee or employer if there are questions. Sometimes direct communication can resolve uncertainties more efficiently than written notes.
- Keep a copy. Always keep a copy of the submitted form for records and future reference.
- Leave sections incomplete. Failing to provide all the requested information can delay the employee’s return to work.
- Assume details are understood without explanation. Do not overlook the importance of specifying the nature of restrictions or the ability to perform job functions.
- Include unnecessary personal or sensitive information. Stick to the details strictly necessary for the form’s purpose and comply with privacy laws.
- Use medical jargon without clarification. Keep language accessible to ensure understanding by all parties involved.
- Rush through the form. Taking the time to fill it out properly can prevent miscommunications and errors.
- Forget to provide contact information for follow-up questions. Both the healthcare provider and the employer may have additional questions or need clarification.
- Ignore the form's instructions. Each section has specific instructions for a reason, ensuring the form is filled out correctly and efficiently.
- Overlook the importance of the return-to-work date. This date is crucial for the employer's planning and should be accurately provided.
- Submit the form without reviewing it with the employee. The employee should be aware of all the information being submitted on their behalf.
- Delay sending the completed form. Timely submission is key to facilitating a smooth return-to-work process.
Misconceptions
Understanding the Return to Work Medical Certification form is essential for both employers and employees. However, several misconceptions surrounding its use and requirements can create confusion. Here are eight common misunderstandings and the correct information for each.
- The form is only necessary for physical health conditions. This is not true. The form can also be used for mental health conditions that have necessitated a leave of absence under the Family and Medical Leave Act (FMLA).
- Employers can demand detailed medical information through this form. Actually, the form is designed to limit the information provided to only that which is necessary to determine the employee’s ability to return to work, avoiding the violation of privacy laws.
- Employees who are on leave don't need to complete the form until they return. In fact, the form should be completed and returned to the employer or department contact listed in Section I prior to the employee's return to work date to ensure a smooth transition.
- The form automatically approves the employee to return to their original job. This is a misconception. Completion of the form merely provides medical certification of the employee's ability to return to work. Whether they return to their original role or another position may depend on the restrictions outlined by the healthcare provider.
- Any healthcare provider can sign off on the form. While many healthcare providers are qualified to complete the form, it's important that they are familiar with the employee's serious health condition and are licensed to practice.
- Genetic information is required for the form’s completion. This is incorrect. Under the Genetic Information Nondiscrimination Act of 2008 (GINA), employers should not request or require genetic information when collecting medical data for the form.
- The form is a one-time requirement. This might not necessarily be the case. If an employee requires extended leave or experiences another serious health condition, a new form may be required to certify each separate instance of leave and return to work.
- The employee determines the return-to-work date. Actually, the return-to-work date is determined based on the healthcare provider’s assessment and indicated on the form. It represents the healthcare provider's professional opinion on when the employee can safely return to work.
Dispelling these misconceptions ensures that both employers and employees can navigate the return to work process more effectively, complying with legal requirements and supporting a healthy work environment.
Key takeaways
The Return to Work Medical Certification form plays a crucial role in managing an employee's transition back to work after taking leave due to a serious health condition. Understanding how to properly fill out and use this form ensures a smooth and compliant process for both employers and employees. Here are five key takeaways to keep in mind:
- Clear communication between the employer and the healthcare provider is essential. The form starts with the employer providing basic information about the employee and the department contact person. This initial step ensures that the healthcare provider knows exactly where and to whom to send the completed form.
- The importance of privacy is underscored by the inclusion of the Genetic Information Nondiscrimination Act (GINA) of 2008 notice. It reminds healthcare providers to avoid sharing any genetic information of the employee or their family members, protecting the employee's privacy.
- Understanding whether an employee is able to perform essential job functions without or with restrictions is paramount. This part not only addresses the employee's current condition but also directly impacts the planning for their return. It determines whether adjustments or accommodations are needed to facilitate a successful transition back to work.
- Specifying whether the provided restrictions are permanent or temporary helps in setting clear expectations and timelines for recovery and accommodation. This detail is crucial for both the employer in terms of workflow management and the employee for personal and professional planning purposes.
- The form must be completed and returned to the appropriate department contact or the employee before the expected return-to-work date. This ensures that all necessary adjustments or accommodations are in place in time for the employee's return, promoting a smoother reintegration into the work environment.
Effectively using the Return to Work Medical Certification form aids in creating a supportive and compliant framework for welcoming employees back to work after medical leave. It highlights the collaborative effort required from employers, employees, and healthcare providers to achieve a successful transition.
Popular PDF Forms
Bill Payment Processing Center Po Box 7236 Sioux Falls - Provides a method for users to notify FIS of their preferred payment mode, including essential bank account information.
Change Name on Marriage Certificate California - Amending records with the VS 24 C form involves a comprehensive review of the current information, precise modifications, and verification by witnesses.
Madison County Al Probate Records - The collaboration between grantors and grantees in filling out this form is a testament to the form’s role in facilitating clear property transactions.