Blank Soc 821 PDF Template
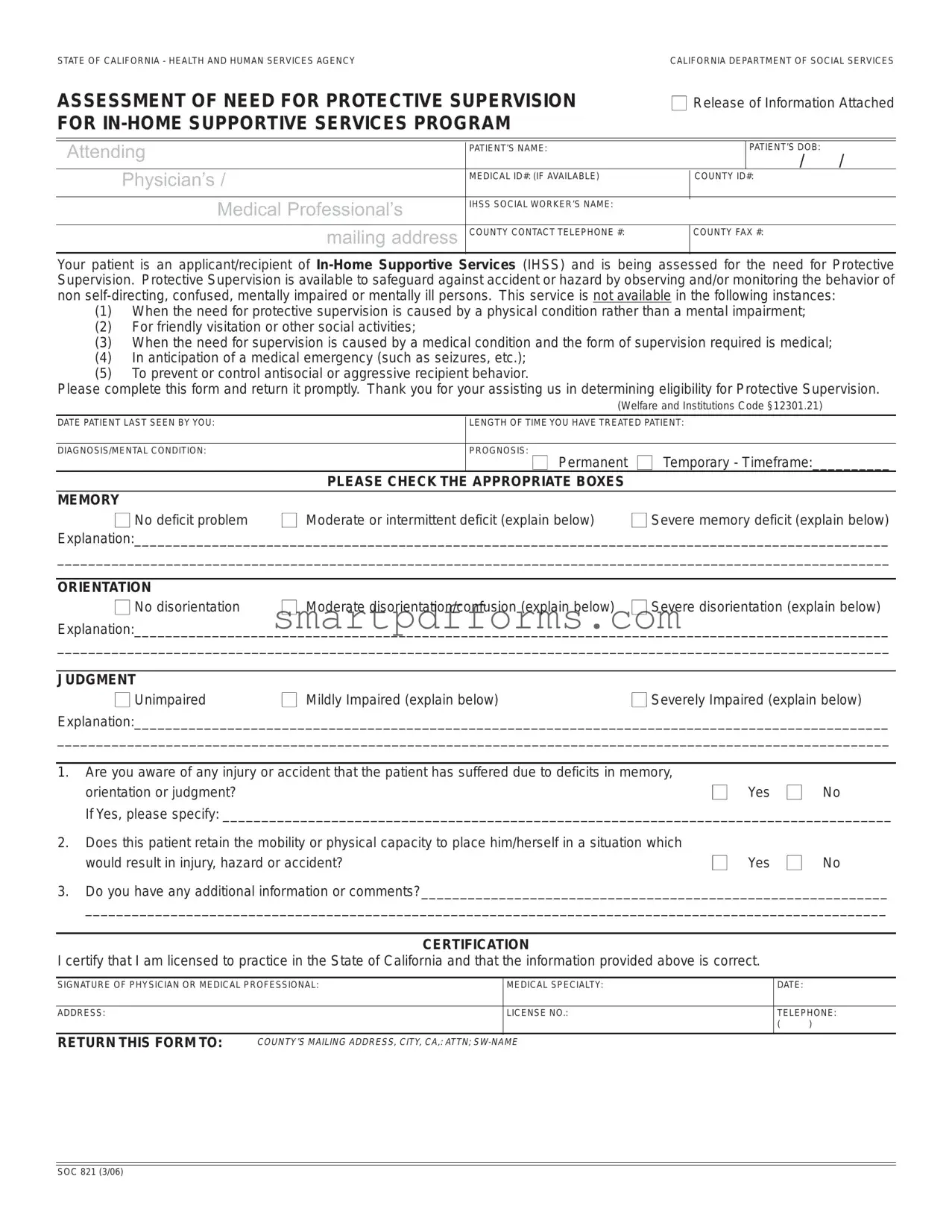
In the realm of supportive care, particularly within California's Health and Human Services Agency, the SOC 821 form represents a critical component in the evaluation process for individuals requiring In-Home Supportive Services (IHSS). This detailed assessment aims to ascertain the need for Protective Supervision for those who are non self-directing, confused, mentally impaired, or mentally ill, ensuring they are safeguarded against potential accidents or hazards due to their condition. The form serves as a bridge between medical professionals and social workers, facilitating a comprehensive review of the patient's medical and mental health status, memory, orientation, judgment, and any history of accidents or injuries incurred due to their condition. It explicitly outlines the circumstances under which Protective Supervision is not provided, such as situations stemming from physical rather than mental impairments, the need for medical rather than supervisory care, and conditions requiring merely social interaction. By requiring a physician’s or medical professional's detailed input regarding the patient’s mental condition, prognosis, and specific needs, the SOC 821 form plays an indispensable role in determining eligibility for Protective Supervision under the IHSS program, thereby highlighting the state's commitment to supporting its most vulnerable populations.
Preview - Soc 821 Form
STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCYCALIFORNIA DEPARTMENT OF SOCIAL SERVICES
ASSESSMENT OF NEED FOR PROTECTIVE SUPERVISION |
■ Release of Information Attached |
|||||
FOR |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Attending |
|
|
PATIENT’S NAME: |
|
|
PATIENT’S DOB: |
|
|
|
|
|
|
/ / |
Physician’s / |
|
MEDICAL ID#: (IF AVAILABLE) |
|
COUNTY ID#: |
||
|
|
|
|
|||
|
|
|
|
|
|
|
|
Medical Professional’s |
IHSS SOCIAL WORKER’S NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
mailing address |
COUNTY CONTACT TELEPHONE #: |
|
COUNTY FAX #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Your patient is an applicant/recipient of
(1)When the need for protective supervision is caused by a physical condition rather than a mental impairment;
(2)For friendly visitation or other social activities;
(3)When the need for supervision is caused by a medical condition and the form of supervision required is medical;
(4)In anticipation of a medical emergency (such as seizures, etc.);
(5)To prevent or control antisocial or aggressive recipient behavior.
Please complete this form and return it promptly. Thank you for your assisting us in determining eligibility for Protective Supervision.
(Welfare and Institutions Code §12301.21)
DATE PATIENT LAST SEEN BY YOU: |
|
LENGTH OF TIME YOU HAVE TREATED PATIENT: |
|
|
|
|
|
DIAGNOSIS/MENTAL CONDITION: |
|
PROGNOSIS: ■ Permanent |
■ Temporary - Timeframe:__________ |
|
PLEASE CHECK THE APPROPRIATE BOXES |
|
|
MEMORY |
|
|
|
■ No deficit problem |
■ Moderate or intermittent deficit (explain below) |
■ Severe memory deficit (explain below) |
|
Explanation:_________________________________________________________________________________________________
___________________________________________________________________________________________________________
ORIENTATION |
|
■ No disorientation |
■ Moderate disorientation/confusion (explain below) ■ Severe disorientation (explain below) |
Explanation:_________________________________________________________________________________________________
___________________________________________________________________________________________________________
JUDGMENT |
|
|
■ Unimpaired |
■ Mildly Impaired (explain below) |
■ Severely Impaired (explain below) |
Explanation:_________________________________________________________________________________________________
___________________________________________________________________________________________________________
1.Are you aware of any injury or accident that the patient has suffered due to deficits in memory,
orientation or judgment?■ Yes ■ No
If Yes, please specify: ______________________________________________________________________________________
2.Does this patient retain the mobility or physical capacity to place him/herself in a situation which
would result in injury, hazard or accident? |
■ |
Yes ■ |
No |
3.Do you have any additional information or comments?____________________________________________________________
_______________________________________________________________________________________________________
CERTIFICATION
I certify that I am licensed to practice in the State of California and that the information provided above is correct.
SIGNATURE OF PHYSICIAN OR MEDICAL PROFESSIONAL: |
MEDICAL SPECIALTY: |
DATE: |
|
|
|
|
|
ADDRESS: |
LICENSE NO.: |
TELEPHONE: |
|
|
|
( |
) |
|
|
|
|
RETURN THIS FORM TO:
COUNTY’S MAILING ADDRESS, CITY, CA,: ATTN;
SOC 821 (3/06)
Form Data
| Fact Name | Description |
|---|---|
| Form Purpose | The SOC 821 form is used in the State of California for the assessment of the need for Protective Supervision under the In-Home Supportive Services (IHSS) Program. |
| Eligibility Criteria | Protective Supervision is aimed at individuals who are non self-directing, confused, mentally impaired, or mentally ill to safeguard against accidents or hazards. |
| Exclusions | The service is not available for needs caused by a physical condition, social activities, medical supervision, anticipation of medical emergencies, or to control antisocial behavior. |
| Required Information | Physicians or medical professionals must provide details on the patient’s memory, orientation, judgment, and any incidents of injury due to these deficits, along with their mobility to self-harm. |
| Governing Law | The form and its processes are governed by the Welfare and Institutions Code §12301.21 of the State of California. |
| Certification Requirement | A physician or medical professional must certify the form, confirming their licensure in California and the accuracy of the information provided. |
Instructions on Utilizing Soc 821
Once it's determined that an individual applying for or receiving In-Home Supportive Services (IHSS) in California may need Protective Supervision because of mental impairments, confusion, or other specific conditions that don't include physical ailments, the SOC 821 form comes into play. This essential document helps in evaluating the requirement for Protective Supervision to ensure the individual's safety against accidents, hazards, or self-injury due to mental incapacity. Understanding and correctly filling out this form is crucial for physicians or medical professionals who are treating the patient. Here's how to do it step by step:
- Fill in the Patient Information Section:
- Write the patient's full name.
- Enter the patient's date of birth (DOB) in the format MM/DD/YYYY.
- Provide the patient's Medical ID number if available, along with the COUNTY ID number.
- Complete the Attending Physician or Medical Professional Details:
- Include your full mailing address.
- Write your name, contact telephone number, and fax number.
- Fill in the IHSS Social Worker’s name associated with the patient.
- Provide Assessment Details:
- Note the date the patient was last seen by you.
- Enter the length of time you have been treating the patient.
- State the patient's diagnosis/mental condition, and select if the prognosis is Permanent or Temporary. If Temporary, specify the timeframe.
- Evaluate and Record Specific Deficits:
- Check the appropriate boxes and provide explanations for the patient's memory, orientation, and judgment abilities.
- Injury or Accident Assessment:
- Indicate whether the patient has suffered any injury or accident due to the aforementioned deficits.
- If yes, specify the details.
- Mobility and Physical Capacity:
- Confirm if the patient retains mobility or physical capacity that could pose a risk to themselves.
- Additional Comments:
- Provide any additional information or comments that could support the assessment.
- Certification:
- Sign the form to certify your assessment is accurate. Include your medical specialty, the date, and your contact information.
- Ensure to fill in your license number and address clearly.
- Return the Form:
- Send the completed form to the specified county mailing address, attention to the SW (Social Worker) with their name, as noted in the form's instructions.
Accurately completing and promptly returning the SOC 821 form plays a pivotal role in ensuring the safety and well-being of individuals under the IHSS program who are unable to protect themselves due to mental impairments. This thorough documentation process aids IHSS in crafting a supportive environment that caters to the specific needs of vulnerable individuals.
Obtain Answers on Soc 821
- What is the SOC 821 form?
The SOC 821 form is a document used by the California Department of Social Services within the In-Home Supportive Services (IHSS) program. Its primary purpose is to assess the need for Protective Supervision for individuals who are non self-directing, confused, mentally impaired, or mentally ill. Protective Supervision aims to safeguard these individuals from accidents or hazards by monitoring their behavior.
- Who needs to complete the SOC 821 form?
This form should be completed by a licensed physician or medical professional who has been treating the patient. It is essential for determining the patient's eligibility for Protective Supervision under the IHSS program.
- What information is required on the SOC 821 form?
The form requires detailed information about the patient, including their name, date of birth, medical ID number (if available), and the name of their IHSS social worker. It also requires the medical professional's diagnosis of the patient’s mental condition, information on memory deficits, orientation, judgment, and any physical abilities that could lead to injury. Furthermore, the medical professional must report any known injuries or accidents suffered by the patient related to their condition.
- Are there any conditions under which Protective Supervision is not available?
Yes, Protective Supervision is not available in several instances, including when the need is caused by a physical condition rather than a mental impairment, for friendly visitation or social activities, when supervision required is medical in nature, in anticipation of a medical emergency, or to prevent/control antisocial or aggressive behavior.
- How should the form be submitted?
After completion, the SOC 821 form should be promptly returned to the county's mailing address provided on the form, attention to the specified social worker (SW-NAME).
- What is the significance of the certification section on the SOC 821 form?
The certification section is crucial as it verifies the legitimacy of the information provided. The medical professional must certify that they are licensed to practice in the State of California and that all the information they have provided on the form is accurate. This includes their signature, medical specialty, date, address, license number, and telephone number.
- What happens after the form is submitted?
Once the SOC 821 form is submitted, the IHSS program reviews the information to determine the patient's eligibility for Protective Supervision. This evaluation process ensures that individuals who are at risk due to mental impairments can receive the necessary supervision to maintain their safety at home.
- How does the diagnosis impact the provision of Protective Supervision?
The diagnosis and details provided about the patient's mental condition, memory, orientation, and judgment play a critical role in determining the need and eligibility for Protective Supervision. A diagnosis indicating severe deficits or impairments is likely to strengthen the case for the necessity of Protective Supervision to prevent accidents or hazards.
- Is there support available for completing the SOC 821 form?
Physicians or medical professionals who have questions about completing the SOC 821 form or need assistance can contact the patient's IHSS social worker or the county office for guidance. This support ensures accurate and thorough completion of the form, aiding in the prompt assessment of the patient's need for Protective Supervision.
Common mistakes
When completing the SOC 821 form, which is crucial for assessing the need for Protective Supervision under the In-Home Supportive Services (IHSS) program, individuals often make mistakes. It's important to fill this form out correctly to ensure that the applicant's needs are appropriately evaluated. Below are seven common errors:
Failing to attach the required Release of Information form can lead to a processing delay or even the inability to evaluate the need for services.
Not specifying the patient's diagnosis or mental condition with enough detail. This information is vital for determining eligibility and the type of supervision required.
Omitting the date the patient was last seen, which helps establish the currency of the medical evaluation and the ongoing nature of the condition.
Leaving the prognosis section blank or not indicating whether the condition is permanent or temporary. This affects the determination of the supervision's duration and nature.
Overlooking the necessity to explain any deficits in memory, orientation, or judgment marked as moderate or severe. Detailed explanations support the need for protective supervision.
Not answering whether the patient has had any injury or accident due to their condition or if they retain the mobility that could result in a dangerous situation. These answers are crucial for assessing risk.
Forgetting to certify the form by signing it and providing the physician or medical professional’s license number, which is essential for the form's validity.
In conclusion, carefully reviewing and providing complete and accurate information on the SOC 821 form is imperative. This ensures that individuals who require protective supervision receive the consideration and services necessary for their safety and wellbeing. Avoiding these common mistakes can significantly streamline the application process for everyone involved.
Documents used along the form
When individuals apply for the In-Home Supportive Services (IHSS) Program, particularly for Protective Supervision due to mental impairments, the SOC 821 form is a crucial document. However, to build a comprehensive support plan, other forms and documents often accompany the SOC 821 form. These additional forms aid in painting a full picture of the applicant's needs, ensuring that they receive the appropriate level of care and supervision.
- SOC 833 - Time Sheet for In-Home Supportive Services: This document is used by care providers to record the hours worked, ensuring they are compensated accurately for the services they provide.
- PA 600 - Application for Public Assistance: Often used in conjunction with SOC 821 to apply for various public assistance programs, furnishing financial support and further services.
- SOC 341 - Report of Suspected Dependent Adult/Elder Abuse: If there's suspicion of abuse, this form is essential for reporting such concerns to protect individuals under IHSS.
- SOC 847 - Consent for Release of Information: This permits the sharing of pertinent information between healthcare providers, and legal or social services, aiding in the care and support plan development.
- MC 210 - Medi-Cal Application: For many IHSS applicants, Medi-Cal eligibility is a prerequisite, and this application is crucial for determining qualifications for healthcare benefits.
- SOC 862 - Rights and Responsibilities: This document outlines the rights of the IHSS recipient and the responsibilities of the IHSS provider, establishing clear expectations for both parties.
- SOC 869 - Personal Health Care Plan: Created by the recipient's physician, this form details the medical care and daily living assistance required, harmonizing it with the caregiver's duties.
- SOC 400 - Provider Enrollment Agreement: Caregivers must complete this agreement to become authorized IHSS providers, ensuring they understand the program's expectations and standards.
- CDSS 835 - Health Care Certification: This form certifies a recipient's health condition and need for IHSS, complementing the SOC 821's assessment of need for protective supervision.
Together, these forms constitute a thorough vetting process that helps identify and fulfill the specific needs of IHSS recipients. Each document plays a unique role in ensuring that individuals receive the care, supervision, and support necessary for them to live safely and comfortably within their homes. This comprehensive approach facilitates a cooperative network of services, healthcare providers, and legal entities all working together to support some of the most vulnerable members of the community.
Similar forms
Form I-9, Employment Eligibility Verification: Similar to the SOC 821 form, Form I-9 is employed within the United States to verify the identity and employment authorization of individuals hired for employment. Both forms are integral to ensuring the eligibility and suitability of individuals within a regulated framework, focusing on verification processes through documentation.
Form SS-5, Application for a Social Security Card: The SOC 821 form shares similarities with Form SS-5 as both involve the collection of personal information and are used to access essential services. Form SS-5 is employed to assign or replace a Social Security Number (SSN), critical for accessing a range of services and benefits, much like how the SOC 821 form is used within the In-Home Supportive Services Program.
Medicare Enrollment Application: Both the SOC 821 and Medicare Enrollment Applications are tied to healthcare services, where the former assesses the need for protective supervision and the latter is used for enrolling in Medicare benefits. Each form plays a pivotal role in ensuring individuals receive the necessary healthcare services and support.
Form 1040, U.S. Individual Income Tax Return: While primarily used for tax filing purposes, Form 1040 and the SOC 821 share the fundamental aspect of collecting detailed personal information for compliance and eligibility determination purposes within federal and state programs.
Advance Healthcare Directive Form: This form and SOC 821 both deal with healthcare decisions, albeit in different contexts. The Advance Healthcare Directive allows individuals to outline their healthcare wishes, while the SOC 821 form assesses a patient's need for protective supervision, both aiming to ensure patient care is aligned with needs and wishes.
DS-11, Application for a U.S. Passport: The application process for a U.S. Passport via the DS-11 form shares similarities with the SOC 821 in terms of gathering personal and sensitive information to determine eligibility for a government-provided service, in this case, international travel authorization versus in-home support services.
HUD-1 Settlement Statement: While the HUD-1 Settlement Statement is utilized in real estate transactions, it shares with the SOC 821 the characteristic of assembling detailed information necessary for official review and documentation purposes in regulatory contexts.
FAFSA (Free Application for Federal Student Aid): Both the SOC 821 form and FAFSA require detailed personal and financial information to determine eligibility for benefits—a protective supervision program in the former and financial aid for education in the latter.
VA Form 10-10EZ, Application for Health Benefits: This form is used by veterans to apply for health benefits through the Department of Veterans Affairs, similar to how SOC 821 is used to apply for protective supervision. Both forms facilitate access to essential health-related services and require thorough personal information.
Medicaid Application Form: The process of applying for Medicaid, which provides health coverage to millions of Americans, including some low-income people, families and children, pregnant women, the elderly, and people with disabilities, necessitates providing detailed personal and health information, a process mirrored by the SOC 821 form's requirements for assessing eligibility for protective supervision within the IHSS program.
Dos and Don'ts
When filling out the SOC 821 form for the State of California's In-Home Supportive Services Program, it is important to follow specific guidelines to ensure the form is completed accurately and efficiently. Here are some key do's and don'ts:
- Do ensure all personal information for the patient is accurate and complete. This includes the patient's name, date of birth, medical ID number if available, and county ID number.
- Do provide thorough explanations for the patient's memory, orientation, and judgment conditions. Just checking a box is not enough; detailed explanations help in assessing the need for protective supervision.
- Do specify if the patient's condition is permanent or temporary, and if temporary, provide an expected timeframe for the condition.
- Do accurately report any incidents of injury or accidents caused by the patient's deficits in memory, orientation, or judgment.
- Don't leave sections incomplete. If a question does not apply, indicate this clearly rather than skipping the section.
- Don't submit the form without the certification section completed, including the signature of the physician or medical professional, their medical specialty, date, and license number.
- Don't forget to provide your contact information accurately, including telephone and the correct mailing address for returning the form.
Adhering to these guidelines ensures the SOC 821 form is filled out comprehensively and increases the chances of the patient being accurately assessed for eligibility for Protective Supervision under the IHSS Program.
Misconceptions
When it comes to understanding the SOC 821 form, several misconceptions are common. This form is crucial for the assessment of need for Protective Supervision under the In-Home Supportive Services (IHSS) program in California. Let's clarify some widely held but incorrect beliefs.
Misconception #1: The SOC 821 is only for children. Many people mistakenly believe that Protective Supervision is exclusively for minors. However, the form is designed to assess the need for supervision for individuals of any age who are non self-directing, confused, mentally impaired, or mentally ill, to safeguard them against accidents or hazards.
Misconception #2: Physical conditions qualify for Protective Supervision. Another common misunderstanding is that physical impairments can qualify an individual for Protective Supervision. The SOC 821 form explicitly states that the service is not available when the need for supervision is caused by a physical condition rather than a mental impairment.
Misconception #3: The form can authorize medical care. Some people think that completing the SOC 821 form can lead to authorization of medical care supervision. This is incorrect; the form is strictly for determining eligibility for Protective Supervision, not for medical supervision due to a condition requiring professional medical intervention.
Misconception #4: A diagnosis guarantees eligibility. It's commonly believed that a diagnosis of a mental condition or impairment automatically qualifies someone for Protective Supervision. In reality, the form requires detailed information about the individual's memory, orientation, and judgment deficits to determine eligibility, not just a diagnosis.
Misconception #5: The SOC 821 form is all that's needed for IHSS application. While critical, the SOC 821 is just one part of the IHSS application process. Applicants need a comprehensive evaluation that includes this form but also involves other documentation and assessments to establish the full spectrum of the applicant's needs.
Misconception #6: The form assesses the need for friendly visitation. Lastly, there's a misconception that the SOC 821 is used to assess the need for social activities or friendly visitation. The form, however, states that Protective Supervision is not available for these purposes, focusing instead on safeguarding those with mental impairments against risks.
Understanding the SOC 821 form and its purpose is crucial for healthcare providers and families seeking Protective Supervision under California's IHSS program. Dispelling these misconceptions can help ensure that those in need receive the appropriate support and supervision.
Key takeaways
When filling out and using the SOC 821 form for the assessment of need for Protective Supervision in the In-Home Supportive Services (IHSS) program, here are key takeaways to consider:
- Collect accurate patient information: Begin by ensuring you have the correct patient name, date of birth, and any applicable medical or county ID numbers. Accuracy in these details is crucial for the proper processing of the form.
- Understand the purpose of Protective Supervision: Protective Supervision is specifically designed to observe and monitor individuals who are non self-directing, confused, mentally impaired, or mentally ill, to safeguard against accidents or hazards. It's important to note the scenarios where Protective Supervision is not applicable, such as physical conditions, medical supervision needs, or social visitation purposes.
- Detail the patient’s condition: Provide a thorough explanation of the patient's mental condition, including memory deficits, disorientation, and judgment impairment. Be clear and detailed, as this will inform the eligibility for Protective Supervision.
- Document significant incidents: If the patient has experienced any injuries or accidents due to their mental condition, it's critical to document these incidents. This information supports the need for protective supervision.
- Assess the patient’s mobility: Evaluate whether the patient retains the physical capacity to place themselves in potentially hazardous situations. This assessment helps in understanding the level of supervision required.
- Provide additional information: If there are other relevant details about the patient’s condition or circumstances that might affect their need for Protective Supervision, include these comments in the designated section on the form.
- Ensure professional certification: The form must be signed by a licensed medical professional, certifying the accuracy of the information provided. This certification is a crucial step for the form's acceptance and the subsequent eligibility determination.
Correctly filling out and submitting the SOC 821 form is vital for assessing a patient's eligibility for Protective Supervision under the IHSS program. Following these key points will aid in the accurate and efficient processing of the form.
Popular PDF Forms
Caregiver Authorization Affidavit - Through this affidavit, the legal system acknowledges the reality of various caregiving scenarios and offers a practical solution.
Capital One Voided Check - Designed by Capital One, this form is a testament to the bank’s commitment to facilitating efficient financial transactions.