Blank Witness Dpa Card PDF Template
In today's healthcare environment, it's crucial for individuals to express their medical wishes clearly, especially when it comes to life-sustaining treatments and end-of-life care. The Witness Dpa Card form serves as a vital tool for members of the Jehovah’s Witnesses community, allowing them to articulate their healthcare preferences in accordance with their religious beliefs. This form not only designates a health-care agent to make decisions on behalf of the individual in the event of incapacitation but also emphatically refuses any blood transfusions, regardless of the situation. This refusal is rooted in the religious convictions of Jehovah’s Witnesses and is a critical component of the document. Additionally, the form provides options regarding the prolongation of life under dire medical circumstances and outlines a space for other health-related instructions, ensuring that all aspects of one's care are addressed. The requirement of witness signatures, including that of a patient advocate or ombudsman for those in skilled nursing facilities, underscores the importance of verifying the individual's intent, soundness of mind, and freedom from undue influence. Furthermore, the form details the specific conditions under which an appointed health-care agent can act, and it emphasizes the need for these roles not to be filled by anyone professionally caring for the individual, to avoid conflicts of interest. Through this document, members of the Jehovah’s Witnesses can ensure that their medical care respects their faith and personal wishes.
Preview - Witness Dpa Card Form
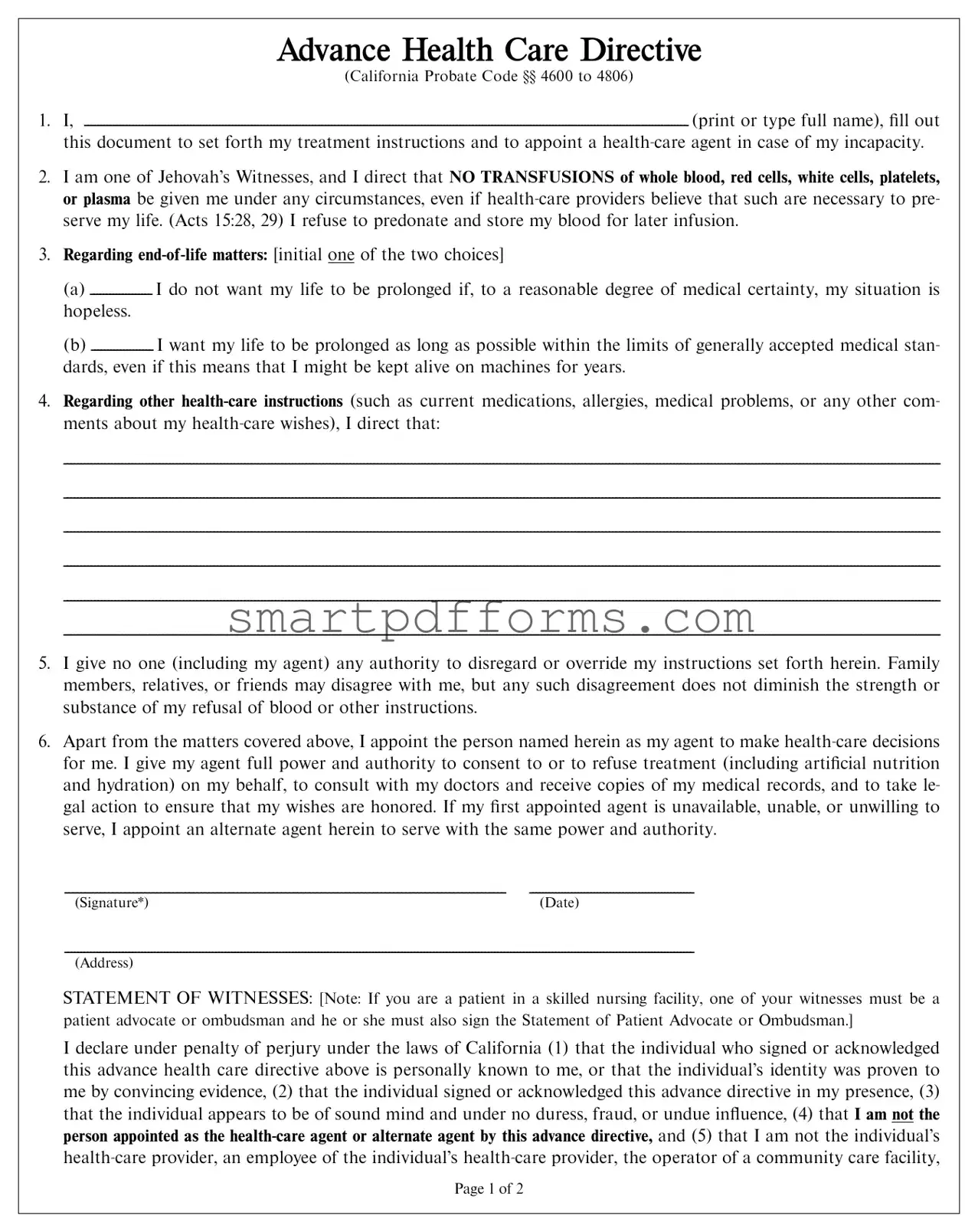
ADVANCE HEALTH CARE DIRECTIVE
(California Probate Code §§ 4600 to 4806)
1.I,
(print or type full name), fill out this document to set forth my treatment instructions and to appoint a
2.I am one of Jehovah’s Witnesses, and I direct that NO TRANSFUSIONS of whole blood, red cells, white cells, platelets, or plasma be given me under any circumstances, even if
3.Regarding
(a) I do not want my life to be prolonged if, to a reasonable degree of medical certainty, my situation is hopeless.
(b) I want my life to be prolonged as long as possible within the limits of generally accepted medical stan- dards, even if this means that I might be kept alive on machines for years.
4.Regarding other
5.I give no one (including my agent) any authority to disregard or override my instructions set forth herein. Family members, relatives, or friends may disagree with me, but any such disagreement does not diminish the strength or substance of my refusal of blood or other instructions.
6.Apart from the matters covered above, I appoint the person named herein as my agent to make
|
|
(Signature*) |
(Date) |
(Address)
STATEMENT OF WITNESSES: [Note: If you are a patient in a skilled nursing facility, one of your witnesses must be a patient advocate or ombudsman and he or she must also sign the Statement of Patient Advocate or Ombudsman.]
I declare under penalty of perjury under the laws of California (1) that the individual who signed or acknowledged this advance health care directive above is personally known to me, or that the individual’s identity was proven to me by convincing evidence, (2) that the individual signed or acknowledged this advance directive in my presence, (3) that the individual appears to be of sound mind and under no duress, fraud, or undue influence, (4) that I am not the person appointed as the
Page 1 of 2
an employee of an operator of a community care facility, the operator of a residential care facility for the elderly, nor an employee of an operator of a residential care facility for the elderly.
|
|
(Signature of witness / Date) |
(Signature of witness / Date) |
|
|
(Address) |
(Address) |
ADDITIONAL STATEMENT OF WITNESSES: At least one of the above witnesses must also sign the following declaration:
I further declare under penalty of perjury under the laws of California that I am not related to the individual execut- ing this advance health care directive by blood, marriage, or adoption, and to the best of my knowledge, I am not en- titled to any part of the individual’s estate upon his or her death under a will now existing or by operation of law.
|
|
(Signature) |
(Signature) |
SPECIAL WITNESS REQUIREMENT: If you are a patient in a skilled nursing facility, you must have the patient advocate or ombudsman also sign the following statement:
STATEMENT OF PATIENT ADVOCATE OR OMBUDSMAN
I declare under penalty of perjury under the laws of California that I am a patient advocate or ombudsman as designat- ed by the State Department of Aging and that I am serving as a witness as required by Section 4675 of the Probate Code.
(Signature of patient advocate or ombudsman / Date)
Name:
Address:
Telephone(s):
(Printed name and address)
*Note: Before signing this document, fill out the entire document (including the names, addresses, and telephone numbers of your
ALTERNATE
Name:
Address:
Telephone(s):
ADVANCE HEALTH CARE DIRECTIVE
(signed document inside)
NO BLOOD
Page 2 of 2 |
Form Data
| Fact Name | Description |
|---|---|
| Governing Law | This form is governed by California Probate Code §§ 4600 to 4806, which outlines the state's specific regulations for advance health care directives. |
| Purpose of the Document | The document allows individuals to set forth their treatment instructions and appoint a health-care agent in the event of their incapacity. |
| Specific Medical Instructions | It explicitly states that no transfusions of whole blood, red cells, white cells, platelets, or plasma be given under any circumstances, in alignment with the beliefs of Jehovah’s Witnesses. |
| End-of-Life Choices | Individuals can instruct whether they desire to prolong their life as long as possible or not to prolong life in hopeless situations, reflecting their personal wishes for end-of-life care. |
| Selection of Health-Care Agent | The form enables the appointment of a health-care agent and an alternate agent, granting them the power to make health-care decisions, including the refusal or consent of treatment, on the individual's behalf. |
| Witness Requirement | Two witnesses must sign the directive, attesting to the sound mind of the signer and noting that they are neither the health-care agent nor have significant conflicts of interest, such as being a healthcare provider or relative who stands to inherit from the signer. |
Instructions on Utilizing Witness Dpa Card
Completing the Witness DPA (Durable Power of Attorney) Card form is a vital step in ensuring your healthcare wishes are respected, especially in critical situations where you might not be able to communicate your desires. This document allows you to appoint a healthcare agent who will have the authority to make decisions on your behalf, in line with the preferences you've outlined. Additionally, it includes specific instructions regarding your health care, such as directives on blood transfusion, which is particularly important for individuals with certain beliefs. To ensure the form accurately reflects your wishes and is legally recognized, following these steps carefully is crucial.
- Fill in your full name at the beginning of the document to indicate that you are the principal creating this advance healthcare directive.
- Specify your directive regarding blood transfusions by acknowledging that no transfusions of whole blood, red cells, white cells, platelets, or plasma be given under any circumstances, in line with your beliefs.
- Choose and initial one of the two end-of-life matter options:
- a) Indicating you do not want your life to be prolonged in hopeless situations, or
- b) Indicating you wish for your life to be prolonged as long as possible within generally accepted medical standards.
- Provide additional health-care instructions such as information on current medications, allergies, medical problems, or your general health care wishes.
- Clearly state that you are giving no authority for anyone (including your agent) to disregard or override the instructions set forth in this document.
- Appoint your health care agent by filling out their full name, address, and telephone number(s), granting them the authority to make health-care decisions on your behalf.
- If desired, appoint an alternate health-care agent by providing their full name, address, and telephone number(s), to serve if the primary agent is unavailable.
- Sign and date the document in the presence of two witnesses, who must then also sign and date the form, confirming they meet the criteria stated. Except under certain circumstances, witnesses can't be the appointed health-care agent(s), your health-care provider, or any employees of a health-care facility you are receiving care from.
- If you are a patient in a skilled nursing facility, ensure a patient advocate or ombudsman signs the form confirming their role and that they witnessed your signature.
After completing the form, share a copy with your appointed health care agent(s), family members who might be involved in your care, and your healthcare providers to ensure everyone is aware of your directives. Keeping a copy in an easily accessible place at home is also wise. This form is a legally binding document that ensures your health care preferences are honored, making its thorough and accurate completion of paramount importance.
Obtain Answers on Witness Dpa Card
-
What is the purpose of the Witness Dpa Card form?
This document serves as an advance health care directive, specifically tailored for individuals who are Jehovah’s Witnesses. It allows a person to outline their health care preferences, including the refusal of blood transfusions under any circumstances. It also enables the appointment of a health-care agent to make decisions on their behalf in case they become incapacitated.
-
Who can be appointed as a health-care agent through this form?
An individual can appoint any adult as their health-care agent except for their supervising health-care provider, an operator or employee of the community care or residential care facility where the individual is receiving care, unless the employee is a relative or coworker. If under conservatorship, a lawyer's consultation is required.
-
What are the key instructions included in the form regarding medical treatment?
The form specifies the refusal of any blood transfusions, regardless of the circumstances. It also addresses end-of-life decisions, providing options regarding the prolongation of life through medical interventions. Furthermore, it includes a section for any additional health-care instructions, such as current medications and allergies.
-
Who needs to witness the signing of the advance health care directive?
The form must be signed in the presence of two witnesses who declare the individual appears of sound mind and not under duress or undue influence. Witnesses cannot be the health-care agent, related to, or entitled to any part of the individual’s estate. If the individual is in a skilled nursing facility, a patient advocate or ombudsman must also sign as a witness.
-
Can family members override the decisions made in this form?
No, the directive gives no authority to anyone, including the designated agent, to disregard or override the instructions set forth in the document. It emphasizes that the refusal of blood transfusions or other specific instructions must be honored, regardless of any disagreements from family, friends, or others.
-
How can the appointed health-care agent utilize this document?
The appointed health-care agent is granted full power and authority to make health-care decisions on the individual’s behalf, including consenting to or refusing treatment and receiving medical records. The agent can also take legal action to ensure the individual’s health care instructions are followed as specified in the document.
Common mistakes
-
Not fully completing the form. Many people skip sections they find confusing or that require additional information they may not have on hand. Every section is important to ensure your health care wishes are understood and met.
-
Choosing a health-care agent or alternate agent who is not reliable or reachable. It's crucial that these individuals are trustworthy and easily contacted in an emergency.
-
Forgetting to update the form. Life changes such as new diagnoses, treatments preferences, or changes in your personal relationships can affect your advance directive. Regular review and updates are necessary.
-
Failing to specify details regarding end-of-life care. Vague instructions can lead to confusion and unwanted medical treatments. Be as clear and specific as possible about your wishes.
-
Not discussing the contents of the form with the appointed agent(s). Ensure your appointed agent understands your wishes and is willing to advocate for them.
-
Misunderstanding the witness requirements. The form has specific rules about who can and cannot serve as a witness, which are often overlooked or misunderstood.
-
Incorrectly assuming family members can override your wishes. The document clearly states no one, including family, can disregard your instructions, but people often fail to communicate this aspect effectively.
-
Not securing the document properly. Many individuals do not keep the document accessible or fail to provide copies to appropriate parties, which can render it ineffective in an emergency.
Common mistakes made can profoundly impact the effectiveness of an advance health care directive. Clear completion, ongoing communication, and proper distribution are key elements to ensure your health care preferences are honored.
Documents used along the form
When preparing for medical decisions and end-of-life care, it's crucial to consider various legal forms beyond the Witness Dpa Card to ensure your wishes are followed. These documents work together to provide a comprehensive plan for your healthcare and personal matters if you're unable to make decisions for yourself. Here are several key forms and documents often used in conjunction with the Witness Dpa Card form:
- Living Will: This document lets you outline your preferences for medical treatments in end-of-life situations or if you're unable to communicate your desires. It can specify which procedures you want to avoid.
- Medical Power of Attorney (POA): Also known as a healthcare proxy, this designates a person to make medical decisions on your behalf if you're incapacitated. It complements the advance healthcare directive by appointing a trusted individual to speak for you.
- Durable Power of Attorney for Finances: This allows a person you choose to manage your financial affairs if you're unable to do so. It can cover actions like paying bills, managing investments, and selling property.
- Physician Orders for Life-Sustaining Treatment (POLST): A POLST form provides medical orders regarding your treatment preferences in various scenarios, typically for seriously ill patients. It's designed to be followed by healthcare providers.
- Do Not Resuscitate (DNR) Order: A DNR instructs medical staff not to perform CPR if your heart stops or if you stop breathing. This document is crucial for individuals who want to avoid life-prolonging treatments.
- Organ and Tissue Donation Registration: This form specifies your intentions regarding organ donation upon death. You can detail which organs and tissues can be donated and for what purposes.
- Last Will and Testament: Although not directly related to healthcare, your last will outlines how you want your assets distributed after your death and can include funeral arrangements, thereby indirectly affecting your end-of-life care.
- HIPAA Release Form: The Health Insurance Portability and Accountability Act (HIPAA) protects your medical information. A release form allows specified individuals to access your medical records, making it easier for family or proxies to make informed decisions.
- Emergency Contact Information Form: While not a legally binding document, listing your emergency contacts, along with their relationship to you, ensures that family members or friends are promptly notified in an emergency.
- Post-Mortem Instructions: Separate from a will, this document provides instructions for handling your body and any ceremonies after your death, reflecting personal, religious, or cultural beliefs.
Creating a comprehensive set of these documents ensures that your healthcare preferences and personal matters are handled according to your wishes, providing peace of mind for you and your loved ones. Consulting with legal and medical professionals can help clarify which documents are essential for your particular circumstances.
Similar forms
Living Will: Similar to the Witness DPA Card, a Living Will articulates personal wishes regarding medical treatment, especially concerning end-of-life care. Both documents are instrumental in guiding healthcare providers when the individual cannot communicate their preferences.
Healthcare Power of Attorney (POA): This legal document, like the Witness DPA Card, involves appointing another person (an agent) to make healthcare decisions on one’s behalf. Both empower the agent to consult with doctors and access medical records, ensuring the principal's healthcare wishes are respected.
Durable Power of Attorney for Health Care: Similar to the healthcare component of the Witness DPA Card, this gives an agent authority over health-related decisions. The key similarity lies in empowering someone else to make medical decisions that align with the individual's wishes when they can't make those decisions themselves.
Do Not Resuscitate (DNR) Order: While more specific in scope, a DNR order shares the Witness DPA Card's purpose by directing medical personnel regarding a specific type of medical intervention – in this case, not to perform CPR. Both documents guide healthcare providers in adhering to the patient’s wishes.
Physician Orders for Life-Sustaining Treatment (POLST): Similar to the Witness DPA Card, a POLST outlines specific instructions for healthcare providers about end-of-life care, including treatments one wishes to avoid. Both are designed to ensure that an individual's healthcare preferences are known and honored.
Medical Orders for Scope of Treatment (MOST): Like the Witness DPA Card, a MOST provides detailed instructions for healthcare providers regarding the scope of treatments to be used or avoided, particularly focusing on patients with serious illnesses, ensuring their healthcare preferences are respected.
Advance Care Plan: This plan, like the Witness DPA Card, outlines an individual's preferences for future healthcare, including treatments they do or do not want. It serves a similar purpose in guiding healthcare decisions when the individual cannot.
Advance Directive: An overarching term that includes elements present in the Witness DPA Card, such as a living will and a healthcare power of attorney. It conveys an individual's wishes regarding medical treatment and appoints an agent to act on their behalf.
Patient Advocate Designation: Similar to parts of the Witness DPA Card, this designates someone to make medical decisions on one’s behalf, underlining the importance of having an advocate to ensure healthcare wishes are followed when one cannot express them.
Five Wishes Document: Like the Witness DPA Card, the Five Wishes Document addresses personal, spiritual, and medical wishes at the end of life. It combines elements of a living will and a healthcare POA, outlining how one wishes to be treated, comforted, and remembered.
Dos and Don'ts
Filling out a Witness Dpa Card form, particularly an Advanced Health Care Directive, requires careful attention to detail and an understanding of its implications. Here are some guidelines to help individuals navigate this process.
- Do ensure that all personal information is accurate and complete. This includes your full name, address, and details of your healthcare agent.
- Don't leave any fields blank unless the form instructs you to do so. If a section does not apply to you, consider writing 'N/A' (not applicable) to clarify that you haven't simply overlooked it.
- Do take your time to understand each section of the form. This document deals with crucial health care decisions, including your stance on blood transfusions and life support.
- Don't forget to initial your choice regarding end-of-life care to clearly indicate your wishes.
- Do appoint a trusted individual as your health-care agent who aligns with your values and understands your wishes. This person will have the authority to make health-care decisions on your behalf.
- Don't appoint your supervising health-care provider, or anyone involved professionally in your residential care, as your agent unless they are related to you. This prevents potential conflicts of interest.
- Do review the witness requirements carefully. If you are a patient in a skilled nursing facility, ensure a patient advocate or ombudsman signs your form as required.
- Don't sign the document without having two witnesses present. Witnesses must also meet specific criteria—they cannot be your health care agent or be related to you by blood, marriage, or adoption.
- Do consult with a legal professional if you have any doubts or require clarification. This is especially important if you are under a conservatorship or have unique circumstances surrounding your health care decisions.
Approaching the Advanced Health Care Directive with thoughtfulness and precision ensures that your health care wishes are honored and legally documented. Remember, this document can be updated as your wishes or circumstances change, so review it periodically with your health care agent and lawyer.
Misconceptions
Many believe the Witness DPA (Durable Power of Attorney) Card is only for religious reasons due to its association with Jehovah’s Witnesses. However, while it includes specific directives about blood transfusions based on religious beliefs, its primary function is to outline all medical preferences and appoint a health-care agent.
There's a misconception that the card grants the appointed agent the power to make all health decisions, disregarding the wishes of the individual. In reality, the card specifies that the agent is to follow the directives provided by the individual, not to override them.
Some assume that once signed, the directives on the Witness DPA Card cannot be changed. That's not the case; individuals can update their instructions as they see fit, ensuring their health care preferences are always current.
It's often misunderstood that the Witness DPA Card is universally recognized and followed by all health-care providers. Though it holds significant legal weight in California, adherence may vary based on individuals' locations and specific health-care provider policies.
Another misconception is that the Witness DPA Card eliminates the need for any verbal communication about health-care wishes. Despite having the card, open discussions with health-care agents and providers are crucial to ensure everyone understands the individual’s preferences.
People sometimes believe that the witness requirements are optional or a mere formality. However, these requirements are legally mandated to ensure the document’s validity and must be taken seriously.
There’s a belief that any family member can serve as a witness. In truth, witnesses must not be the health-care provider, an employee of a health-care institution where the individual is receiving care, or anyone entitled to a portion of the individual's estate upon their death, unless meeting specific exceptions.
Some think the card only covers decisions related to end-of-life care. While it does include directives for such situations, it also allows for instructions on a range of medical decisions and the appointment of a health-care agent.
Many are under the impression that the Witness DPA Card is valid in all states once signed in California. In practice, its validity outside of California may vary depending on each state’s laws regarding advance directives and health-care powers of attorney.
Lastly, there's a misconception that a lawyer must be involved in the creation or execution of the Witness DPA Card. While consulting a lawyer can be beneficial, especially for complex situations, it is not a requirement for the card to be valid.
Key takeaways
Filling out an Advance Health Care Directive (AHCD) form is a critical step in ensuring your health care preferences are honored, especially for individuals with specific beliefs or health care instructions due to their faith, as seen in the Witness Dpa Card form for Jehovah’s Witnesses. Here are key takeaways you should consider while filling out and using this form:
- Clarify Your Treatment Preferences: It is imperative to specify your medical treatment preferences, including the refusal of specific interventions such as blood transfusions, to ensure they are respected regardless of the situation.
- Appoint a Health-Care Agent: Selecting a trusted individual to act as your health-care agent allows them to make health-care decisions on your behalf if you are unable to do so. Make sure this person understands your beliefs and wishes thoroughly.
- Consider End-of-Life Decisions: Clearly state your preferences regarding end-of-life care, including the extent to which you wish to receive treatment and under what conditions you would prefer to withhold or withdraw treatment.
- Include Detailed Health-Care Instructions: Providing additional instructions concerning your current medications, allergies, and any medical problems can be invaluable in ensuring that your health care is managed according to your wishes.
- Authority of Your Decisions: Emphasize that your instructions are final and cannot be overridden by anyone, including family members or the appointed health-care agent, ensuring that your health-care preferences are followed.
- Select a Secondary Agent: Appointing an alternate agent is wise in case your primary choice is unavailable or unable to serve, ensuring there is always someone available to advocate for your health-care decisions.
- Witness Requirements: The document must be signed in the presence of two witnesses who confirm your identity, your voluntary execution of the document, and your capacity to make health-care decisions. Certain individuals are prohibited from serving as witnesses to avoid conflicts of interest.
- Special Considerations for Skilled Nursing Facility Patients: If you are a patient in a skilled nursing facility, one of your witnesses must be a patient advocate or ombudsman, underscoring the importance of unbiased witnessing in such settings.
It's essential to communicate your health-care desires clearly and ensure that your AHCD reflects your current decisions. Regularly reviewing and updating your AHCD is recommended to ensure that it continually matches your preferences and legal requirements.