Blank Ymca Member Cancellation Letter PDF Template
When deciding to terminate a membership with the YMCA, an individual steps into a process that is both a rite of passage and a formal goodbye to a community that often extends beyond fitness into personal development and social networking. The YMCA Member Cancellation Letter plays a crucial role in this process, serving as the official notice to the organization of a member's intent to end their affiliation. This document, although straightforward, carries weight, symbolizing the end of an association with an institution known for its commitment to building healthier and more connected communities. It's a procedure that requires attention to detail, adherence to the specific YMCA's policy on cancellations, and an understanding of the potential impact on one's access to the YMCA's facilities and programs. Crafting this letter with care ensures that the process of disengagement is smooth, leaving the door open for future reconnection while respectfully closing the current chapter of one's YMCA membership journey.
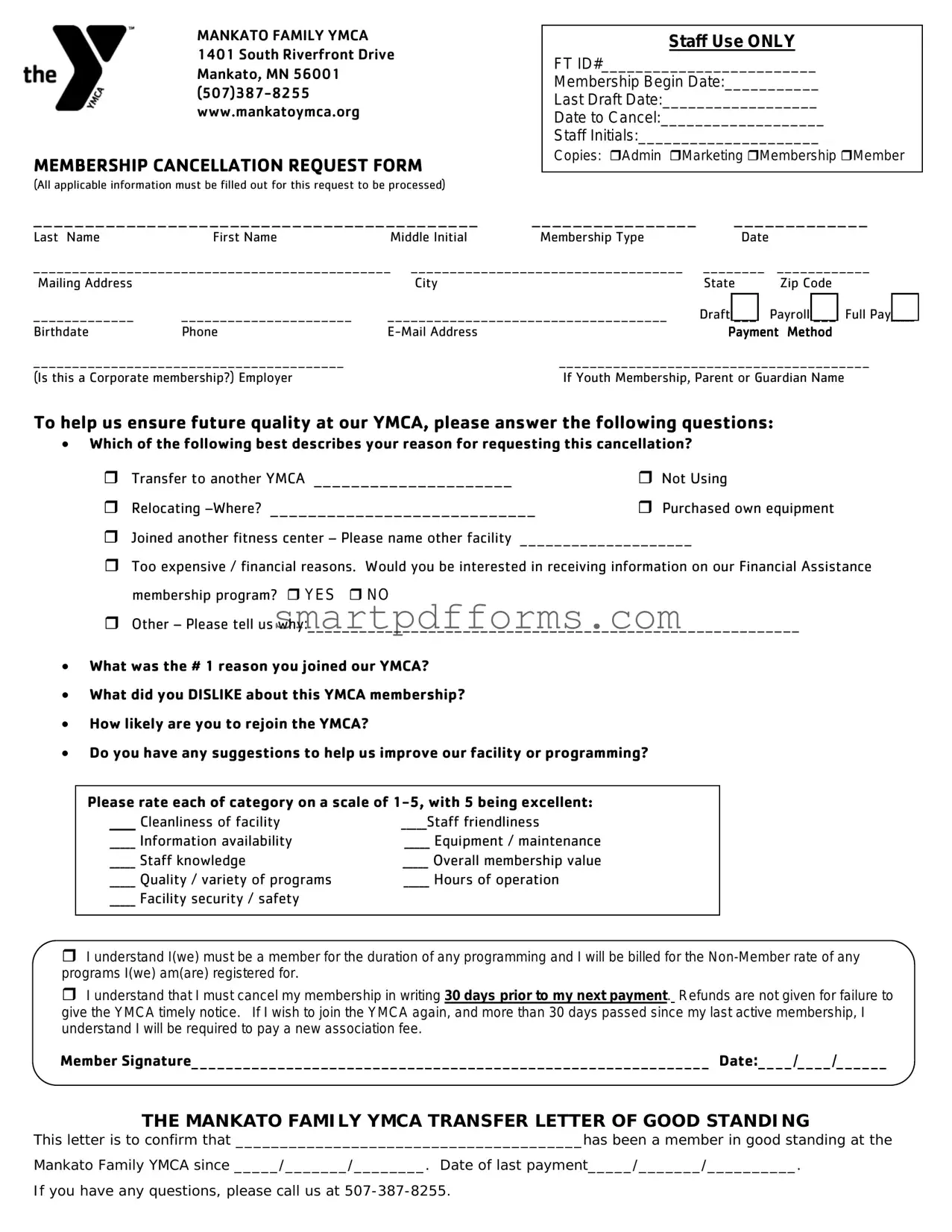
Preview - Ymca Member Cancellation Letter Form
MANKATO FAMILY YMCA 1401 South Riverfront Drive Mankato, MN 56001
MEMBERSHIP CANCELLATION REQUEST FORM
(All applicable information must be filled out for this request to be processed)
Staff Use ONLY
FT ID#_________________________
Membership Begin Date:___________
Last Draft Date:__________________
Date to Cancel:___________________
Staff Initials:_____________________
Copies: Admin Marketing Membership Member
___________________________________________ |
________________ |
_____________ |
|||
Last Name |
First Name |
Middle Initial |
Membership Type |
Date |
|
______________________________________________ ___________________________________ |
________ |
____________ |
|||
Mailing Address |
|
City |
|
State |
Zip Code |
_____________ |
______________________ |
____________________________________ |
Draft ___ |
Payroll ___ Full Pay_____ |
|
Birthdate |
Phone |
|
Payment Method |
||
________________________________________ |
|
________________________________________ |
|||
(Is this a Corporate membership?) Employer |
|
If Youth Membership, Parent or Guardian Name |
|||
To help us ensure future quality at our YMCA, please answer the following questions:
•Which of the following best describes your reason for requesting this cancellation?
|
Transfer to another YMCA _____________________ |
Not Using |
|
Relocating |
Purchased own equipment |
Joined another fitness center – Please name other facility ____________________
Too expensive / financial reasons. Would you be interested in receiving information on our Financial Assistance membership program? YES NO
Other – Please tell us why:_________________________________________________________
•What was the # 1 reason you joined our YMCA?
•What did you DISLIKE about this YMCA membership?
•How likely are you to rejoin the YMCA?
•Do you have any suggestions to help us improve our facility or programming?
Please rate each of category on a scale of
_____ Cleanliness of facility |
_____Staff friendliness |
_____ Information availability |
_____ Equipment / maintenance |
_____ Staff knowledge |
_____ Overall membership value |
_____ Quality / variety of programs |
_____ Hours of operation |
_____ Facility security / safety |
|
I understand I(we) must be a member for the duration of any programming and I will be billed for the
I understand that I must cancel my membership in writing 30 days prior to my next payment. Refunds are not given for failure to give the YMCA timely notice. If I wish to join the YMCA again, and more than 30 days passed since my last active membership, I understand I will be required to pay a new association fee.
Member Signature____________________________________________________________ Date:____/____/______
THE MANKATO FAMILY YMCA TRANSFER LETTER OF GOOD STANDING
This letter is to confirm that _______________________________________has been a member in good standing at the
Mankato Family YMCA since _____/_______/________. Date of last payment_____/_______/__________.
If you have any questions, please call us at
Form Data
| Fact Number | Description |
|---|---|
| 1 | The YMCA Member Cancellation Letter form is used by members who wish to terminate their YMCA membership. |
| 2 | Most YMCAs require written notice, often 30 days in advance, to cancel a membership. |
| 3 | Some state laws may impact the cancellation process, including notice periods and refunds. |
| 4 | The form typically asks for member information such as name, address, and membership number. |
| 5 | A reason for cancellation may be requested but is not always required. |
| 6 | Submitting the form does not guarantee cancellation until confirmed by the YMCA. |
| 7 | Members should keep a copy of the cancellation letter and any confirmation received for their records. |
| 8 | In some cases, members may cancel in person or via email, depending on the YMCA’s policies. |
| 9 | Governing laws vary by state, affecting cancellation rights, refunds, and notice periods. |
Instructions on Utilizing Ymca Member Cancellation Letter
When deciding to end your membership with the YMCA, it's essential to communicate your intention clearly and formally through a cancellation letter. This process involves providing specific details to ensure your request is processed smoothly. By following a structured format, you can create a comprehensive letter that covers all necessary information, helping to facilitate a hassle-free cancellation. Here's a step-by-step guide to completing your YMCA Member Cancellation Letter form effectively.
- Start with your contact information. At the top of the letter, include your full name, address, phone number, and email address to make sure the YMCA can reach you if needed.
- Include the date. Below your contact information, write the current date to mark when the cancellation request was made.
- Address the letter properly. Direct your letter to the appropriate department or individual, using the format "To Whom It May Concern" if you're unsure of the exact recipient.
- Write a clear opening statement. In the first paragraph, clearly state your intention to cancel your YMCA membership, including your membership number for reference.
- Specify the reason for cancellation (optional). While not mandatory, providing a reason for your cancellation can offer valuable feedback to the YMCA.
- List any applicable details. If there are specific conditions related to your cancellation, such as a medical issue or relocation, mention these in your letter.
- Request confirmation. Politely ask for a written confirmation of your membership cancellation to ensure that your request has been processed.
- Express appreciation. It's courteous to thank the organization for the services or experiences you've had during your membership.
- Close with your signature. End the letter by signing your name, which indicates the letter's authenticity and your agreement to the terms of cancellation.
- Provide copies of relevant documents. If your cancellation requires supporting documents (e.g., medical documentation or proof of relocation), attach copies to your letter.
After submitting your YMCA Member Cancellation Letter, it's advisable to follow up if you have not received a confirmation within a reasonable timeframe. This ensures your request has been received and is being processed. Taking this step can help avoid any misunderstandings or delays in ending your YMCA membership.
Obtain Answers on Ymca Member Cancellation Letter
What is a YMCA Member Cancellation Letter form?
This form is a document used by members who wish to cancel their memberships with the YMCA. It provides a formal way to notify the YMCA of the member's intention to end their membership, ensuring the process is handled properly.
Why do I need to submit a cancellation letter to the YMCA?
Submitting a cancellation letter is necessary to officially start the process of canceling your membership. It serves as a formal request and ensures that your cancellation is processed in accordance with YMCA policies.
What information do I need to include in the cancellation letter?
The letter should include your full name, membership ID or account number, address, phone number, and the effective date of cancellation. Additionally, you may explain your reason for cancellation, though it is not always required.
How do I submit my YMCA Member Cancellation Letter?
By mail: Send your signed letter to the address of your local YMCA branch.
In person: Deliver your letter directly to a staff member at your local YMCA.
Email: Some branches may allow you to send your cancellation letter via email. Check with your local YMCA for their specific policies.
Is there a specific format I should follow?
While there's not a one-size-fits-all format, your cancellation letter should be clear and concise, containing all the necessary personal information and your request to cancel the membership. Using a polite and formal tone is also advisable.
Can I cancel my YMCA membership online?
Whether you can cancel online depends on your local YMCA's policies. Some branches may offer online cancellation forms or accept cancellation requests via their website. It’s best to check directly with your local branch for this information.
How soon will my membership be cancelled after I submit the letter?
Processing times can vary by location. Typically, it may take up to 30 days for your cancellation to be fully processed. For specific timelines, please contact your local YMCA directly.
Will I receive a confirmation of my membership cancellation?
Yes, you should receive a confirmation once your membership cancellation has been processed. If you haven’t received any confirmation within a few weeks of submission, it’s a good idea to follow up with the YMCA.
Are there any fees associated with cancelling my YMCA membership?
Fees for canceling a membership vary depending on your YMCA’s policies and the terms of your membership agreement. Some locations may require a cancellation fee or have specific conditions under which fees are waived. Always check with your local YMCA for detailed information on any applicable fees.
Common mistakes
-
Not providing detailed personal information is a common error. It's essential to include full name, membership ID, and contact details. This allows the YMCA to accurately identify your account and process the cancellation.
-
Failing to specify the cancellation date can lead to misunderstandings. Members should clearly state when they wish for their membership to end, taking note of any requirements for notice periods.
-
Omitting reasons for cancellation might seem inconsequential, but it is helpful information for the YMCA. Understanding why members choose to cancel can lead to improvements in facilities and services.
-
Lack of a signature can invalidate the entire process. A signature verifies the request's authenticity, making it a crucial component of the cancellation letter.
-
Forgetting to request a confirmation for the cancellation is a mistake. Members should explicitly ask for a confirmation via email or mail to ensure that the cancellation has been processed.
Besides these common errors, here are additional considerations to ensure the cancellation process goes smoothly:
- Check if there are any specific terms stated in your membership agreement regarding cancellations, such as notice periods or fees.
- Keep a copy of the cancellation letter for your records. This can be useful if there are any disputes in the future.
- Ensure the letter is sent through reliable means, such as certified mail, to have proof of delivery.
Documents used along the form
When managing a YMCA membership, various forms and documents may be necessary to ensure all member needs and requests are accurately processed and recorded. The YMCA Member Cancellation Letter is one such document utilized in the process of canceling a membership, but it often works in tandem with other important materials. The documents listed below are commonly associated with the management and cancellation procedures at the YMCA, each serving a specific purpose within the broader context of membership services.
- Membership Application Form: This form initiates the process, gathering personal info, membership type requests, and payment details. It's the beginning of a member’s journey, ultimately leading to the use or cancellation of services.
- Emergency Contact Information: These details are crucial for ensuring member safety and welfare, important to have on file from the start and through any changes in membership status.
- Payment Authorization Form: Sets up automatic billing for membership fees, frequently revisited when updating payment methods or finalizing a cancellation.
- Change of Information Form: Allows members to update their personal information, such as address or phone number, which may be relevant during the cancellation process to ensure all communications are properly directed.
- Hold Request Form: Members might temporarily suspend their membership due to various reasons; this form is often a precursor or alternative to outright cancellation.
- Program Registration Forms: Separate from general membership, these forms enroll members in specific YMCA programs and may affect a member’s decision to maintain or cancel their membership.
- Facility Rental Agreement: For members or organizations that rent YMCA facilities, this agreement outlines the terms and conditions of use, which may need to be concluded or transferred upon membership cancellation.
- Feedback and Survey Forms: After canceling, members are often encouraged to provide feedback on their experience, which helps the YMCA improve its services for current and future members.
- Waiver and Release Forms: Members sign these forms to acknowledge the risks associated with physical activity and facility use, important from enrollment to cancellation for liability reasons.
- Privacy Policy Acknowledgment: Members acknowledge understanding the YMCA’s policies on data use and privacy, crucial as they manage personal information even after cancellation.
Together, these documents encompass a robust system for managing YMCA memberships from start to finish. They ensure that both the organization and its members are fully informed, agreed upon terms of use, and aware of their rights and responsibilities throughout the membership lifecycle, including its cancellation.
Similar forms
Gym Membership Cancellation Letter: This document is very similar because it also serves the purpose of formally requesting the termination of a membership agreement. It typically contains the member’s name, membership number, and a clear request to cancel the membership according to the terms of the agreement.
Subscription Service Cancellation Letter: Much like a membership cancellation letter, this document is used to terminate a recurring service. It must contain specific details such as the subscriber's account information and be directed towards the service provider to formally request the cessation of services.
Insurance Policy Cancellation Letter: This document is used to notify an insurance provider of the policyholder's intention to cancel their insurance policy. It is similar because it legally formalizes the intention to end an ongoing service agreement, often specifying the reason for cancellation and the desired date of termination.
Monthly Subscription Box Cancellation Letter: Similar in intent to other cancellation letters, this letter is specifically directed at companies that offer monthly box subscriptions. It requires the customer's account details and usually a statement of intent to cancel, articulated clearly to avoid any automatic renewals.
Rental Agreement Termination Letter: While this document pertains to a different sector—the real estate sector—it is akin to a membership cancellation letter in its function of formally terminating an agreement. It usually includes a notice period as required by the agreement or law, the date of vacating the premises, and a request for the deposit return.
Service Contract Cancellation Letter: This letter is used to end a service agreement before its natural expiration date. It's similar because it requires a clear statement of intent to cancel, along with any necessary details like account or contract numbers, and often the reasons for cancellation to comply with the service contract’s terms.
Dos and Don'ts
When you decide to cancel your YMCA membership, it's important to do so in a clear and correct manner. To ensure your cancellation process is smooth, follow these guidelines.
Do's when filling out the YMCA Member Cancellation Letter:
- Review your membership agreement to understand the terms of cancellation.
- Include all required personal information, such as your full name, address, and membership ID.
- Specify your reason for cancellation clearly, but keep it brief and to the point.
- Refer to any supporting documents or previous correspondence regarding your cancellation.
- State the effective date of cancellation as per the agreement terms.
- Request a confirmation of cancellation in writing.
- Keep a copy of the cancellation letter for your records.
- Send the letter via certified mail or through a method that provides a delivery confirmation.
- Be polite and professional in your tone, even if you're dissatisfied with the service.
- Contact the YMCA directly to verify they've received your cancellation request.
Don'ts when filling out the YMCA Member Cancellation Letter:
- Don't omit any personal information that may be needed to identify your account.
- Don't be vague about your cancellation request; clearly state your intention to cancel.
- Don't forget to sign the letter, as an unsigned letter may not be processed.
- Don't assume the cancellation is immediate; understand any notice periods.
- Don't send the cancellation letter without keeping a copy for your own documentation.
- Don't use aggressive or confrontational language, regardless of your experiences.
- Don't neglect to confirm receipt of your letter by the YMCA.
- Don't delay sending your cancellation letter, especially if there's a notice period.
- Don't fail to check for any final steps or confirmation needed on your part post-cancellation.
- Don't ignore the importance of reviewing your bank statements for any after-cancellation charges.
Misconceptions
Many people have misconceptions about the process involved in canceling a YMCA membership. Understanding these can help ensure that the process is as smooth as possible.
You can cancel your YMCA membership immediately. This is not always the case. Most YMCA branches require a notice period before the cancellation takes effect. Typically, this is about 30 days, but it varies by location.
Cancellation can only be done in person. While some YMCA locations might prefer in-person cancellations to discuss the decision and possibly offer alternatives, many YMCAs accept cancellation requests via mail, email, or phone.
A cancellation fee must always be paid. This is not a universal requirement. Some branches may charge a fee, but others do not. It's important to check the specific policy of your YMCA.
You don't need to write a cancellation letter if you've already spoken to someone at the YMCA. Even if you've discussed cancelling your membership with a staff member, many YMCAs require a written cancellation to process your request officially.
Any family member can submit the cancellation request. The request must typically be made by the primary member on the account or someone legally authorized to act on their behalf.
The cancellation takes effect the same month it is requested. Due to the notice period, the cancellation may not take effect until the following month. Make sure to plan accordingly.
Your membership will be automatically cancelled if you stop paying the fees. Non-payment does not equal cancellation. In fact, this could lead to additional fees or being sent to collections. Formal cancellation is necessary to officially end membership.
Refunds are provided for the remaining time of the membership. YMCA generally does not provide refunds for any remaining part of the membership period after cancellation. However, policies can vary, so it's advisable to check.
You need to provide a specific reason for cancelling. While providing a reason might be encouraged or requested for internal feedback purposes, it is typically not a requirement for processing your cancellation.
Key takeaways
When members decide to cancel their YMCA membership, it's important to handle the process thoughtfully to ensure a smooth and clear termination of services. Knowing how to properly fill out and use the YMCA Member Cancellation Letter form is vital. Below are key takeaways that will guide members through this process:
- Ensure all membership details are accurate: It’s crucial to include accurate and up-to-date personal information such as full name, membership ID, and contact information. Accuracy in these details helps prevent any delays or issues in processing the cancellation.
- State the reason for cancellation: While not always mandatory, providing a reason for your cancellation can help the YMCA improve its services. Whether it’s due to relocation, financial reasons, or dissatisfaction, being clear and honest can be beneficial.
- Specify the cancellation date: Clearly indicate when you want the cancellation to take effect. This is important for record-keeping and to ensure you are not billed beyond your intended usage.
- Understand the cancellation policy: Familiarize yourself with the YMCA’s cancellation policy beforehand. Policies can vary by location, including notice periods and any applicable cancellation fees.
- Proofread the letter: Before submitting, proofread the letter to ensure all information is correct and that there are no misunderstandings in your request.
- Keep a copy of the letter: After sending, keep a copy of the cancellation letter for your records. This can serve as proof of your request in case there are any discrepancies or if the cancellation is not processed as requested.
- Follow up if necessary: If you don’t receive confirmation of your cancellation within the expected timeframe, follow up with the YMCA. A direct call or visit may be needed to ensure your membership has been successfully canceled.
- Be mindful of the mode of submission: Whether the cancellation letter is accepted via email, mail, or in person can vary. Ensure to send it through the preferred or required method by your YMCA branch.
- Check for a confirmation response: Finally, ensure you receive a confirmation of cancellation from the YMCA. This confirmation is your assurance that you will no longer be billed and that your membership has ended.
By adhering to these guidelines, members can ensure a smoother cancellation process with the YMCA, avoiding any unnecessary complications or misunderstandings.
Popular PDF Forms
Privacy Act Statement for Email - Designed to serve as a reminder of the legal and ethical obligations to protect individuals’ privacy when handling documents containing personal information.
Retention Certificate - From detailed guidelines to the convenience of nominee assignments, the V778 form is designed to make the retention and transfer of registration numbers as straightforward as possible.
Clayton County Superior Court Forms - The structured format for reporting assets and liabilities ensures that all relevant financial information is considered during legal proceedings.